About the rapid response investigation pilot
In 2025, HSSIB undertook a pilot project to test a process for rapid investigation of patient safety issues and to use the learning to help develop HSSIB’s investigation methods. The pilot focused on patient safety issues within a regional system where multiple organisations were involved in providing care across a care pathway.
The nature of the pilot meant that HSSIB had to take a proportionate and pragmatic approach to evidence collection and analysis. The pilot did not explore the same breadth of services as many other HSSIB investigations and did not contain wider, national benchmarking or comparisons. This was to allow a balance between the time and depth of the investigation and to ensure that important safety learning could be shared as soon as possible. HSSIB encouraged the organisations involved to take further action to explore areas highlighted in the pilot where the approach had not allowed for more in-depth analysis.
About this report
This report is for provider organisations, integrated care boards, and specialised commissioners that may be involved in the delivery and commissioning of care pathways across regions in England. It draws on learning from the rapid response investigation pilot and wider learning from HSSIB investigations and other relevant sources.
The report shares safety learning about care pathways across organisational boundaries. It does not share specific details about the care pathway, organisations or commissioners involved in the pilot.
A note of acknowledgement
We would like to thank the many people who contributed across the organisations involved in the rapid response investigation pilot. Their openness demonstrated a willingness to ensure patients in the region receive the best possible care. The investigation would like to offer its thanks to the organisations involved for their participation and willingness to engage in a new safety investigation approach to help inform future HSSIB work.
Executive comment from the provider of the specialist service: Increasingly care pathways span many organisations and while there are numerous benefits for patients and staff that accompany centralisation, we are aware that safety for all users could be impacted by large-scale change and reconfiguration. Working with HSSIB has allowed us to review a critical regional service and ensure that no patient is disaffected by the change. Much of the learning shared by the HSSIB team was known to us and was being addressed when we invited the review, but we welcomed novel insights, the ‘critical friend’ approach, and the opportunity to share our learning more widely across the healthcare system. The report has allowed us to convene a regional summit and work in collaboration with key partner organisations to apportion aspects of our improvement plan.
Executive summary
This report shares learning gained through examination of a regional care pathway – that is, a pathway of assessment and care for patients with a particular health condition – during an HSSIB rapid response investigation pilot.
The investigation aimed to investigate safety concerns shared with HSSIB about the safety and effectiveness of a care pathway that spanned multiple organisations and where specialist services were centralised to a single site. The pathway had been redesigned with engagement from the organisations, the public and staff to reduce inequalities. It was intended to improve patient outcomes and ensure efficient use of resources across the region.
The investigation provided insights into how the governance of care pathways, including oversight and risk management, is achieved, and how cultural and communication challenges between organisations impacted on patients receiving appropriate care. The investigation identified differences between how the redesigned pathway was expected to operate and how it worked in practice. These differences affected staff wellbeing and led to concerns about risks to patient safety, including delays in access to specialist care.
The learning in this report is shared to support organisations and integrated care boards (ICBs) to adopt effective change management processes that are informed by patient safety considerations when designing, implementing and overseeing care pathways.
Findings
- A cross-organisation implementation board oversaw the redesign and initial implementation of the care pathway. Support and oversight from the ICB was time limited, ending before the project had been fully implemented, which impacted on the operationalisation of the service.
- A business case for implementation of the pathway was approved but not fully realised. This created expectations for how the pathway would operate that were not met in practice.
- There was no shared view across organisations about what the redesigned pathway could offer patients in reality. This limited the organisations’ ability to understand the risks across the pathway and to mitigate them to as low as reasonably practicable.
- There was no single guidance document shared between organisations, and there were inconsistencies in the documentation used to support decision making about whether patients should be provided with specialist care.
- Organisations held different perceptions of the risks to patient safety created by the redesign of the pathway. This impacted on clinical decision making and led to disagreements between teams.
- Organisational oversight of the pathway after its implementation was limited due to disengagement among staff and the absence of a collaboratively agreed evaluation plan.
- The data collected about the care pathway differed across organisations and was not routinely shared between them. This led to a difference in understanding about how the care pathway was working in practice and where improvements could be made.
- The ICB had limited ability to support ongoing improvement of the care pathway and had limited access to information about the quality and safety of the pathway in practice.
- Differences in the perceived purpose of the pathway led to barriers to collaborative learning and improvement of the pathway. These included examples of incivility among staff, which is known to impact on staff wellbeing and patient outcomes.
HSSIB suggests safety learning for integrated care boards
HSSIB investigations include safety learning for integrated care boards where this may support the response to a patient safety issue across a geographical area.
Safety learning for integrated care boards ICB/2026/019:
HSSIB suggests that integrated care boards proactively identify the impact of commissioning decisions on pathways prior to implementation and develop mitigations to reduce any potential impacts on patient safety and equitable access to care.
Safety learning for integrated care boards ICB/2026/020:
HSSIB suggests that integrated care boards support organisations to effectively evaluate the implementation of new care pathways.
Local-level learning prompts
HSSIB investigations include local-level learning where this may help organisations and staff identify and think about how to respond to specific patient safety concerns at the local level. HSSIB has developed the following prompts to support local-level learning for NHS trusts when collaborating with other organisations across a regional care pathway.
Safe implementation of the care pathway
- How do you identify and resource dedicated support to implement new care pathways?
- How do you ensure appropriate tools and resources are used to support the design and implementation of the care pathway?
- How do you identify and mitigate unexpected challenges to patient safety arising from the care pathway’s implementation?
- How do you identify and mitigate any mismatch between the expectations of patients, families, carers or staff and what the pathway can deliver in practice?
- How do you ensure that implementation of a care pathway is effectively evaluated to improve safety and learning?
- How do you identify and mitigate potential harm caused when implementing a new care pathway?
The care pathway in practice
- How do you identify and manage incivility between staff across different organisations?
- How do you facilitate shared learning opportunities for staff across different organisations?
- How do you ensure information and documentation used to support the care pathway are aligned across different organisations?
- How do you enable staff to understand the context in which the care pathway may work in different organisations?
- How do you engage staff to understand the different requirements for electronic systems that may exist across the care pathway?
- How do you support interoperability of electronic systems to enable effective information sharing across different organisations?
- How do you enable new technology to be adopted and used across different organisations?
- How do you consider relevant tools and guidance when developing work processes across different organisations?
Oversight of the care pathway
- How do you ensure shared governance forums are appropriately established and resourced, and are effective?
- How do you ensure concerns about the care pathway are escalated and acted on by senior and executive leadership teams across different organisations and the integrated care board?
- How do you ensure consistency in how data is collected and shared across different organisations, including with integrated care boards?
- How do you ensure that risks to the care pathway are identified and mitigated to as low as reasonably practicable across different organisations?
- How do you ensure messages about the care pathway are effectively shared and understood by staff across different organisations?
- How do you identify and facilitate proactive communication with a point of contact at the integrated care board with oversight of the care pathway?
1. Background
This section provides background information about this learning report and regional care pathways. It also includes consideration of other relevant HSSIB and national work.
1.1 Approach to this learning report
1.1.1 The rapid response investigation pilot was intended to test how HSSIB can identify and deliver a response to patient safety concerns in an accelerated way. HSSIB worked with organisations to identify issues to test the approach while also seeking to add value to a regional healthcare system. The pilot ran between August and October 2025.
1.1.2 Following identification of a patient safety concern, the investigation undertook site visits at multiple organisations and engaged with staff at all levels, including executive, managerial, clinical and patient safety staff. The site visits also enabled the investigation to meet patients and follow them through a care pathway. Interviews were held with the integrated care board (ICB) and further information was obtained from relevant local and national policies, guidance and literature. To support the collection and analysis of evidence, the investigation used the Systems Engineering Initiative for Patient Safety (SEIPS) (Carayon et al, 2006; Holden et al, 2013).
1.1.3 On completion of the pilot, HSSIB evaluated its approach to the investigation. HSSIB worked with the organisations involved to share learning about the care pathway and identified an opportunity to share wider learning about regional care pathways. The intention is that this learning can support organisations and ICBs in considering how their own pathways may operate or may be improved to further manage and mitigate risks to patient safety.
1.2 Care pathways
1.2.1 The aim of a care pathway is to enhance the quality of patient care by improving outcomes, promoting patient safety, increasing patient satisfaction, and optimising the use of resources. A care pathway needs to be modelled to meet the needs of patients, and various modelling methodologies exist to help development and implementation (Gartner et al, 2025; du Sartz de Vigneulles et al, 2025).
1.2.2 A care pathway is a complex intervention involving mutual decision making and organisation of care processes for a specific group of patients during a defined period (European Pathways Association, n.d.). The characteristics of a care pathway include:
- an explicit statement of the goals and elements of care based on evidence, best practice, patients’ expectations and their characteristics
- facilitation of communication among team members and with patients and families
- co-ordination of care processes by co-ordinating the roles and activities of the multidisciplinary care team, patients and their relatives
- documentation, monitoring, and evaluation of variances and outcomes.
1.2.3 A range of resources are available to help in the ongoing design, delivery and evaluation of care pathways; these include publications by The Health Foundation (2017a; 2017b) highlighting lessons for redesigning care pathways (see figure 1). Other articles have noted a lack of literature to support how care pathways should be implemented and have gone on to propose new methods to implement, learn, replicate, and scale up care pathways (Gartner et al, 2025).
Figure 1 Ten lessons to support the development and implementation of new care models (The Health Foundation 2017b)

1.3 Regional commissioning of NHS services
1.3.1 In recognition of the need for better care co-ordination across complex health and care pathways, integrated care systems (ICSs) were developed. Their role is to bring together providers and commissioners of NHS services across a geographical area to plan care to meet the needs of the people in that area. ICBs facilitate integration between local healthcare organisations in their ICS. Their role includes commissioning pathways of care within regions to support safe and effective patient care. ICBs also have a role in helping to design patient safety into cross-organisational care pathways and fostering cross-organisational working (Patient Safety Learning, 2023).
1.3.2 In March 2025, NHS England directed ICBs to reduce their operating costs by 50% and to refocus their work on strategic commissioning (NHS England, 2025a). To do this, ICBs were asked to look carefully at functions where there may be duplication with NHS providers or NHS England regional teams, including assurance and regulatory functions and wider performance management.
1.3.3 In May 2025, a model blueprint for ICBs was published by NHS England which set out the ‘direction of travel for their role and functions’ (NHS England, 2025b). This included a desire to improve collaborative working with partners and better use of data and analytics to support more proactive care. In addition, ICBs were asked to:
- commission across pathways of care and increasingly focus on population-based care
- continue to work in partnership to bring together providers to best improve healthcare and the health and wellbeing of their local population.
1.3.4 Some specialised care continues to be commissioned by NHS England and its regional teams. Care commissioned by NHS England was not considered in the pilot.
1.4 Previous relevant HSSIB reports
Safety management
1.4.1 In October 2023, HSSIB (2023) published a report exploring the concept of safety management systems (SMSs) in safety-critical industries. An SMS is a proactive and integrated approach to managing safety. It sets out the structures and accountabilities to be integrated into an organisation’s day-to-day activities. There are four areas associated with many SMS frameworks:
- safety policy – establishes senior management’s commitment to improve safety and outlines responsibilities
- safety risk management – includes the identification of hazards and risks, and their mitigation
- safety assurance – involves the monitoring and measuring of safety performance, and evaluating the effectiveness of implemented risk controls
- safety promotion – includes training, communication and other actions to support a positive safety culture within all levels of the workforce.
1.4.2 The report found that there is an opportunity to improve safety activities in healthcare to increase proactivity and co-ordination across and within organisations. It also found that if there is no co-ordinated approach in place across organisations, accountability and responsibility can become misaligned, leading to gaps in the oversight of safety management.
1.4.3 In February 2025, HSSIB (2025a) published an investigation report on safety management: accountability across organisational boundaries. The report was intended to help improve patient safety in relation to the management of patient safety risks across organisational boundaries. Key findings included:
- there are no overarching principles that all healthcare providers and ICBs can use which enable a consistent and collaborative approach to the management of patient safety
- national organisations’ expectations of how ICBs manage patient safety are not in line with what ICBs can currently achieve due to challenges with resourcing and the usability of safety data
- cross-organisational safety risks are not always being escalated to ICBs and there may be limited resources and capability to identify, define and investigate such risks.
1.4.4 The investigation shared safety learning with ICBs to support them when seeking assurance of how health and care providers will work together when commissioning services.
2. Implementation of the care pathway
This section describes the investigation's findings in relation to how the care pathway was redesigned and implemented, and the associated implications for patient safety. It draws on the evidence gathered from organisations, staff, policy and guidance as outlined in 1.2.
2.1 Redesign of the care pathway
2.1.1 In the early 2020s, a case for change was proposed by commissioners and local organisations to redesign the care pathway with centralisation of specialist services at a single site. The aim of the proposed redesign was to reduce health inequalities, improve patient outcomes, and ensure efficient use of resources. It also aimed to account for several factors that were impacting on existing service provision, including:
- increasing demand caused by changes in local population demographics and more people living with long-term conditions
- variation in access to the specialist service, the care provided and outcomes for people, depending on where they lived
- workforce shortages, particularly in specialist roles, that challenged service delivery and achievement of national standards.
2.1.2 Consultation on the proposed redesign took place through engagement with stakeholders including staff, patients, carers, public representatives and third-sector organisations. It also included a formal public consultation. The consultation process engaged with approximately 500 people during pre-consultation and received over 2,000 responses. This feedback informed the redesign of the care pathway.
2.1.3 Following consultation and planning for the redesign, a business case was developed which set out how changes would be implemented and how the new pathway would operate. The investigation identified that several of the concerns raised about the pathway could be traced back to the implementation phase.
Implementing the care pathway
2.1.4 Implementation of the redesigned pathway progressed over a 3-month period with oversight from a project board and support from subcommittees/task and finish groups. The investigation identified a difference between the expectations for implementation set by the business case and the subsequent operation of the care pathway in reality.
2.1.5 Implementation did not fully proceed as originally intended, with several factors contributing to this difference. These included the complexity of the reconfiguration, concurrent reorganisation of regional commissioning processes, and the continued impact felt by healthcare services in the aftermath of the COVID-19 pandemic.
2.1.6 An important factor was that the business case had modelled that a specific number of beds would be available to provide adequate provision for patient care throughout the care pathway. However, the investigation was told that not all the specified bed numbers had been funded in later decisions made by the integrated care board (ICB). This meant that the bed numbers on which the care pathway was modelled were inaccurate, which impacted on how the pathway could be implemented.
2.1.7 Staff involved in the care pathway told the investigation that the business case had created the expectation “that all patients meeting the [pathway] criteria would be managed via that specialist pathway” and so would all be accepted to go directly to the location of the specialist service. In reality, patients were sometimes declined by the specialist service and instead went to their nearest hospital. This was described as creating a “two-tier system” for patients and was heard to have caused “conflict” between organisations about accepting patients in line with the criteria.
2.1.8 Staff also told the investigation of their expectation that the care pathway would be evaluated after implementation. The business case described that processes would be in place ‘to measure the effectiveness and success of the changes made to services’ and to ‘explore impacts’ at defined points following implementation. The investigation was unable to identify a formal evaluation plan and instead saw that each organisation involved in the pathway was undertaking its own form of evaluation. This is explored further in 4.1.
Patient safety concerns
2.1.9 Staff involved in the pathway described their perceptions that harm to patients was occurring because of the pathway redesign, including delays in patients receiving specialist care. While data suggested that patients may be experiencing some delays in aspects of their care, and staff concerns are an important indicator of potential issues in care, the investigation found limited evidence of actual harm to patients as a result of the redesign.
2.1.10 The limited evidence of reported harm contrasted with what was heard from staff. It was unclear whether this difference was due to limitations in the reporting data, or whether it was representative of negative sentiments towards the redesign of the pathway. Several staff described being angry when patients were not cared for as they would have expected and that this impacted on morale and job satisfaction.
2.2 Learning from the investigation
2.2.1 The investigation found that the initial plans for redesign of the care pathway involved proactive engagement with the local/regional population and focused on improving efficiency, access and safety. This allowed the planning to consider the perspectives of patients and staff, and account for a range of factors relevant to the local population served by the pathway. This approach is in line with a previous HSSIB (2025a) investigation that highlighted the importance of being responsive to the needs of local population groups to mitigate risks to patient safety.
2.2.2 The initial intentions for the redesign of the care pathway were to improve efficiency, access, and safety for patients and staff involved in providing care and accounted for a range of factors relevant to the local population served by the pathway. In the implementation of the care pathway, the investigation found that expectations set by the business case led to assumptions about how the pathway would work in practice. When those expectations were not fully met, this led to the concerns described and perceptions that risks to patient safety created by the implementation had not been mitigated.
2.2.3 Various tools are available to support the design and implementation of care pathways (see 1.2). These tools commonly refer to the need for a staged or phased approach, with continuous review and improvement. Throughout the phases, the tools describe the need to proactively engage staff to develop a shared understanding of future need and how the implementation of the care pathway will be achieved. This includes testing assumptions about a planned implementation and considering mitigations should those assumptions not be realised. Considering these tools and the findings of the investigation, the following learning is shared.
Safety learning for integrated care boards ICB/2026/019:
HSSIB suggests that integrated care boards proactively identify the impact of commissioning decisions on pathways prior to implementation and develop mitigations to reduce any potential impacts on patient safety and equitable access to care.
Safety learning for integrated care boards ICB/2026/020:
HSSIB suggests that integrated care boards support organisations to effectively evaluate the implementation of new care pathways.
Local-level learning
HSSIB investigations include local-level learning where this may help organisations and staff identify and think about how to respond to specific patient safety concerns at the local level. HSSIB has developed the following prompts to support local-level learning for NHS trusts when collaborating with other organisations across a regional care pathway.
Safe implementation of the care pathway
- How do you identify and resource dedicated support to implement new care pathways?
- How do you ensure appropriate tools and resources are used to support the design and implementation of the care pathway?
- How do you identify and mitigate unexpected challenges to patient safety arising from the care pathway’s implementation?
- How do you identify and mitigate any mismatch between the expectations of patients, families, carers or staff and what the pathway can deliver in practice?
- How do you ensure that implementation of a care pathway is effectively evaluated to improve safety and learning?
- How do you identify and mitigate potential harm caused when implementing a new care pathway?
3. The care pathway in practice
This section describes how the regional care pathway worked in practice. It includes consideration of the training, tools and technology components of the surrounding work system - that is, the overall context in which the pathway operates.
3.1 Staff understanding of the pathway
3.1.1 The investigation observed variation in how staff across different organisations interpreted which patients should receive specialist care under the pathway. Staff described differing interpretations of the acceptance criteria in different organisations.
3.1.2 These differing interpretations led to variation and disagreement between staff across organisations about which patients should be accepted, could be accepted, and which patients would be accepted. Some staff described experiencing “pushback” to two-way discussions due to “hostility”, and situations where patients were “bouncing back and fore” between the providers before a decision was made about the care they should receive. This impacted on patients, families and carers by adding confusion and uncertainty to their care.
3.1.3 Disagreements were heard to cause anger, frustration, conflict and, on some occasions, incivility. Incivility is known to have a detrimental impact on staff wellbeing and patient care, and NHS England (n.d.a) provides resources to help address incivility. However, these resources do not directly address how incivility can be dealt with across organisations within a care pathway.
3.1.4 The investigation identified that the differing interpretations of the care pathway and its criteria were influenced by “staff not being on the same page”. A number of factors were seen to impact on the ability of staff, and the organisations, to gain a shared understanding of how the pathway worked in practice. Some of these factors are explored below.
Cross-provider training opportunities
3.1.5 The investigation heard of limited opportunities for cross-provider training during the care pathway’s implementation. This was influenced by the involvement of several geographically spread organisations with large workforces across different specialties.
3.1.6 Staff told the investigation they wanted interorganisational, multidisciplinary training to help develop consistent thinking across the team about the care of patients, including the potential for simulated training across the different provider teams.
3.1.7 The investigation was also told that training plans had been limited during the implementation period and the need for cross-provider training opportunities had only been recognised after implementation, when some of these concerns had become apparent.
Pathway documentation
3.1.8 The investigation heard that the pathway was not consistently followed by all organisations and staff. The investigation found that this was influenced by inconsistencies in how they understood the pathway, and in the guidance and tools used by the different organisations to support safe and effective patient care.
3.1.9 The investigation identified that there was no single guidance document for staff across all organisations to help them follow the care pathway.
The investigation reviewed the supporting documentation for the care pathway available within each organisation. Each had a separate document describing the inclusion and exclusion criteria for patients to enter the pathway and the processes for care from its own perspective. These guidance documents were not shared between organisations to encourage a shared understanding of how the pathway worked ‘end to end’.
3.1.10 The investigation also noted differences between organisations in the patient assessment tools that were used to determine whether a patient should be treated under the care pathway. The investigation identified that different interpretations of the criteria related to which patients “should” be accepted onto the care pathway, and which patients “could” be accepted.
3.1.11 Several statements in the guidance and supporting documents about when specialist care should be provided were also seen to be contradictory. These differences meant that staff in different organisations were sometimes working to different criteria when assessing a patient’s symptoms, which could lead to differences in their conclusions about whether patients should receive specialist care.
3.1.12 The specialist service described that, “ideally”, any patient meeting the criteria would be directly accepted. However, because the criteria were “highly sensitive but not specific”, the service risked being overwhelmed with patients who may later be found not to have needed specialist care. These capacity challenges were not recognised by staff outside of the specialist service; instead, the service was seen to be “refusing” or “rejecting” patients who staff considered eligible.
3.1.13 The investigation heard from staff of the need to clarify for all staff across the organisations the realities of what the care pathway could reasonably deliver considering the resources available. The investigation was also told that the pathway documentation needed to be standardised through a co-designed approach across the organisations involved and include a realistic representation of ‘work-as-done’ – that is, how things actually happen in practice.
Technology and digital systems
3.1.14 The investigation heard about limitations in the technology and digital systems used in support of the care pathway. The business case stated that ‘The whole pathway will be supported by significant digital advancements …’. Staff described that this had not been achieved, with different electronic patient record (EPR) systems operating across the organisations involved, with varying interoperability to support access to patients’ medical histories and previous interactions with healthcare services.
3.1.15 One organisation had its own EPR system that other organisations could not access. Two organisations used the same EPR system, but despite this, there was limited interoperability between the systems to allow information to be easily shared. This meant that across the care pathway, different staff in different organisations had access to different information, with no staff member having access to all the relevant information about a patient’s care.
3.1.16 The investigation was also told about the benefits of other technology to enable specialist staff to support non-specialist staff when assessing patients in different locations. Technology for video consultation had been purchased by two organisations but was not being used. Factors contributing to the situation included limited engagement between the specialist and non-specialist teams to embed its use, varying attitudes towards the value of the technology, and problems with the supporting infrastructure.
3.1.17 Some staff had limited awareness of the existence of this technology and described that while it had been purchased, its use had not been implemented. The technology had become “forgotten about” and staff continued to rely on telephones to communicate about patient care.
3.2 Learning from the investigation
3.2.1 The investigation found that decisions across the care pathway were made by staff within the context of their own organisations to reflect what each thought was the most appropriate approach. However, the investigation also found variation in those decisions and therefore in supporting procedures, leading to conflict between organisations and staff.
3.2.2 Tools for the design and implementation of care pathways describe the importance of understanding the context within which a pathway is being implemented. That context includes the work system and the interactions between elements such as the people involved, environments, technology and inter-organisational processes. Frameworks such as the Systems Engineering Initiative for Patient Safety (SEIPS) can support exploration of work systems and help with proactive planning for design or redesign of a care pathway (Carayon et al, 2006; Holden et al, 2013).
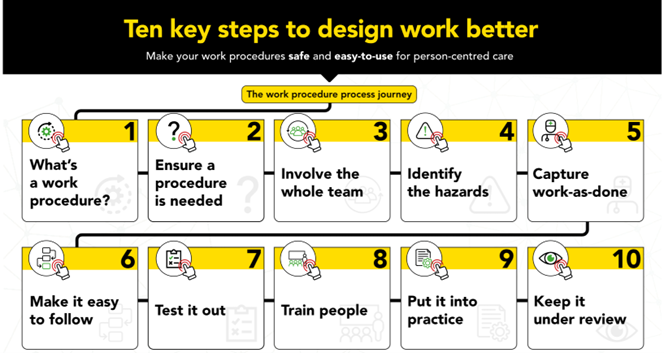
3.2.3 The Chartered Institute of Ergonomics and Human Factors (2020) provides guidance on the design of effective work procedures (see figure 2). The guidance highlights the importance of understanding work-as-done and involving the whole team in development, testing and implementation.
Figure 2 Ten key steps to design work better (Chartered Institute of Ergonomics and Human Factors, 2020)
3.2.4 The 10-year health plan for England sets out the intention for the NHS to move from analogue to digital to help improve care (Department of Health and Social Care, 2025). However, the investigation noted practical challenges that can be faced in adopting technology across care pathways.
3.2.5 Previous HSSIB investigations (for example, 2025b) have commented on the challenges posed to patient care when digital systems are not interoperable and limit information sharing across a care pathway. This report also identified local learning for organisations to support consideration of interoperability when systems are procured and in ongoing monitoring of how digital systems work in practice.
Local-level learning prompts
HSSIB investigations include local-level learning where this may help organisations and staff identify and think about how to respond to specific patient safety concerns at the local level. HSSIB has developed the following prompts to support local-level learning for NHS trusts when collaborating with other organisations across a regional care pathway.
The care pathway in practice
- How do you identify and manage incivility between staff across different organisations?
- How do you facilitate shared learning opportunities for staff across different organisations?
- How do you ensure information and documentation used to support the care pathway are aligned across different organisations?
- How do you enable staff to understand the context in which the care pathway may work in different organisations?
- How do you engage staff to understand the different requirements for electronic systems that may exist across the care pathway?
- How do you support interoperability of electronic systems to enable effective information sharing across different organisations?
- How do you enable new technology to be adopted and used across different organisations?
- How do you consider relevant tools and guidance when developing work processes across different organisations?
4. Oversight of the care pathway
This section describes how governance of the regional care pathway worked in practice, including at organisational and regional levels.
Governance is ‘a system through which NHS organisations are accountable for continuously improving the quality of their services and safeguarding high standards of care …’ (NHS England, n.d.b). Governance systems include oversight – the ongoing monitoring of performance and quality of services – and the processes that provide assurance of patient safety and quality of care.
4.1 Governance across the organisations
4.1.1 Several issues were raised around ongoing oversight, evaluation and assurance of the care pathway. Limited inter-organisational collaboration was described, influenced by disagreements, disengagement and limited capacity of individuals to be involved to represent providers in governance forums.
4.1.2 The investigation mapped the governance structures for the pathway to help understand oversight processes. A clinical oversight group (COG) was intended to provide ‘a clinical and operational oversight and governance function’ on behalf of the integrated care board (ICB). The COG reported and escalated issues to the ICB as required. However, the investigation was told that the COG’s terms of reference did not fully represent how it had been able to operate in practice.
4.1.3 Some of the planned workstreams feeding into the COG to share information had not been established, due to factors such as local funding arrangements. This limited the COG’s ability to provide effective oversight of the pathway and for senior leadership to hear and respond to feedback and concerns about how the pathway was working in practice.
Data collection
4.1.4 The investigation observed that each organisation was collecting some form of data in relation to the pathway. The data collected was from the perspectives of those organisations to “prove” that there was a problem with the pathway or to “assure” that appropriate patients were being accepted into the pathway. The data therefore had different aims. It also used different methodologies/criteria for collection, making it difficult to make comparisons.
4.1.5 Staff across the organisations agreed that the differences in data collection and awareness of results suggested limited oversight of the pathway. They described that organisations and teams worked independently across the pathway and not always in a collaborative way.
4.1.6 The investigation was shown the different data held by each organisation involved in the pathway. However, when discussing the data with the organisations, it was apparent that not all the organisations had access to all the data shared with the investigation. Some of the data had not been presented to the COG which meant a shared understanding of the ‘current state’ of the pathway had not been achieved. When seeing data from other organisations that they had not seen before, some staff described it as “reassuring” as it alleviated some of their concerns about the numbers of patients being declined from the pathway.
Risk management processes
4.1.7 The investigation was told by staff outside of the specialist service that the concerns they had about risks to patient safety had not been heard by senior leadership teams. Some staff described also being told not to challenge situations when patients were declined for the care pathway, and interpreted this as being asked to not raise concerns about patient safety. This further contributed to the negative sentiments towards the pathway and disengagement from its governance.
4.1.8 The investigation explored how risks to patients were identified and mitigated. This was heard to be part of the COG’s responsibilities and had been considered throughout planning, design and implementation. Following implementation, the investigation identified that the issues with disengagement and limited evaluation meant the risks across the pathway had not been fully considered.
4.1.9 Staff in some of the organisations had raised concerns that risks associated with patients not receiving timely access to specialised care could not be eliminated or effectively mitigated due to the design of the current pathway. Because of this, some patients did not receive timely care and there were perceptions that the ‘risk’ was being passed between organisations. It was unclear whether collaborative efforts across the organisations had aimed to understand the risks to patient care and mitigate them to ‘as low as reasonably practicable’ (ALARP). ALARP is a risk concept that involves weighing a risk against the effort, time and money needed to control it.
4.1.10 The investigation found that staff had significant concerns about caring for patients without specialist support. These included concerns about the resource-intensive nature of caring for some patients who staff felt should be on the specialist pathway, and which staff felt took resource away from other patients.
4.1.11 Similarly, staff and organisations involved in providing the pathway’s specialist care were concerned that some patients were escalated to them unnecessarily and that this could impact on patients who they felt were a higher priority for specialist support. This included staff feeling that demand and bed availability influenced decisions about whether to admit patients for specialist care because they “simply don’t have the space to take all [patients]”.
4.1.12 Staff across organisations described a lack of “assurance” – that is, confidence – those risks to patients introduced by implementation of the redesigned pathway had been recognised and mitigated.
4.2 Involvement of the integrated care board
4.2.1 The investigation also explored how the ICB supported organisations involved in the care pathway and oversaw the pathway. The investigation was unable to identify a specific function, role or person at the ICB that was responsible for overseeing the evaluation and ongoing improvement of the care pathway once it had been implemented; this was not included in the business case. This limited the ability for “good relationships” to develop between the organisations and the ICB to encourage effective information sharing, the benefit of which was identified in a previous HSSIB investigation (2025a).
4.2.2 The investigation met with representatives from the ICB operational delivery group. This group’s role was to monitor performance of care pathways and receive escalation of issues from organisations. The group was aware of some of the challenges that had impacted on the implementation of the care pathway, such as the commissioning decisions around the modelled bed numbers. The investigation was unable to determine what engagement or mitigations had been put in place to help limit the impact of these challenges on patient care.
4.2.3 The ICB was not aware of some of the patient safety concerns that were raised to the investigation about the pathway. The operational delivery group described that it would react to safety and quality concerns raised about a care pathway but only sought certain information on a regular basis to monitor performance. This meant the ICB did not have full sight of the concerns about patient safety as these had not been shared with them. These findings echo those of HSSIB’s (2025a) investigation, where HSSIB heard from ICBs that they did not understand the types of patient safety risks that were arising in care pathways because of limited information sharing by organisations.
4.2.4 The organisations involved in the care pathway also shared their perceptions that the ICB had limited ability to support the governance and ongoing improvement of the care pathway. The ICB said it was open to supporting collaboration if it was aware of issues, but also that it was facing challenges itself considering national changes across ICBs. ICBs are being impacted by staffing changes and requests to cut costs, and The King’s Fund (2025) has highlighted that ‘previous experience shows that a focus on cutting costs makes collaboration – key to strategic commissioning – harder’.
4.2.5 The ICB agreed to an HSSIB request for it to convene the organisations at a roundtable meeting, to re-establish relationships and expectations for the safe and effective operation of the care pathway. There was a delay in this meeting being convened due to significant ongoing operational pressures across the providers and changes in the ICB’s structure.
4.2.6 The roundtable was chaired by the ICB and attended by all the organisations involved in the care pathway. HSSIB also attended to provide additional context to the meeting about the investigation’s findings. An action plan to address the learning points was discussed collaboratively, and further actions were allocated to the appropriate organisations to continue the learning and improvement process.
4.2.7 The roundtable highlighted some early improvements, including a notable reduction in incivility, an increase in cross-organisational understanding of care pathway specifics and nuances, and the beginning of work considering digital systems. Other learning had not yet been addressed to the same degree, including digital system solutions and, in relation to governance, where the delivery of oversight mechanisms by the ICB was yet to be defined and resourced due to ongoing restructure challenges.
4.2.8 This reflects the challenges HSSIB has observed at local, regional and national level in relation to effective oversight and governance across boundaries of care, which will be explored further in a future HSSIB report.
4.3 Learning from the investigation
4.3.1 Gaps in the oversight of the pathway, and limited clarity across organisations around the risks to patients from implementation of the redesigned pathway, impacted on the ability to take an effective approach to implementation. Without defining the accountabilities of all stakeholders within the wider health and care system it was challenging for ICBs and providers to understand their role in the management of patient safety. This meant that there was limited opportunity to take a proactive approach to safety risk management or safety assurance, as potential hazards, risks and possible controls to mitigate any risks were not shared across organisations.
4.3.2 The investigation recognises the challenge of engaging and working collaboratively across multiple organisations involved in a care pathway. These challenges were highlighted through the lens of patient safety investigation in HSSIB’s (2025c) report ‘Investigating under the Patient Safety Incident Response Framework (PSIRF): sharing HSSIB learning for future development’. That report described how co-ordinating collaboration across multiple organisations was difficult and ICBs were not always able to provide the support and co-ordination needed.
4.3.3 These challenges are likely to continue at a national level given the current reorganisation of NHS England with the Department of Health and Social Care. While reorganisation is intended to reduce running costs and avoid duplication of functions (NHS England, 2025a), there is an impact on ensuring appropriate staff and services are available and able to take action to help drive improvements in patient safety.
Local-level learning
HSSIB investigations include local-level learning where this may help organisations and staff identify and think about how to respond to specific patient safety concerns at the local level. HSSIB has developed the following prompts to support local-level learning for NHS trusts when collaborating with other organisations across a regional care pathway.
Oversight of the care pathway
- How do you ensure shared governance forums are appropriately established and resourced, and are effective?
- How do you ensure concerns about the care pathway are escalated and acted on by senior and executive leadership teams across different organisations and the integrated care board?
- How do you ensure consistency in how data is collected and shared across different organisations, including with integrated care boards?
- How do you ensure that risks to the care pathway are identified and mitigated to as low as reasonably practicable across different organisations?
- How do you ensure messages about the care pathway are effectively shared and understood by staff across different organisations?
- How do you identify and facilitate proactive communication with a point of contact at the integrated care board with oversight of the care pathway?
5. References
Carayon, P., Schoofs Hundt, A., et al. (2006) Work system design for patient safety: the SEIPS model, BMJ Quality & Safety, 15(Suppl 1), i50–i58. doi: 10.1136/qshc.2005.015842
Chartered Institute of Ergonomics and Human Factors (2020) Guidance on design of effective work procedures. Available at https://ergonomics.org.uk/resource/guidance-on-design-of-effective-work-procedures.html (Accessed 9 March 2026).
Department of Health and Social Care (2025) 10 Year Health Plan for England: fit for the future. Available at https://www.gov.uk/government/publications/10-year-health-plan-for-england-fit-for-the-future (Accessed 9 March 2026).
European Pathways Association (n.d.) About care pathways. Available at https://e-p-a.org/care-pathways/ (Accessed 9 March 2026).
Gartner, J.B., Lemaire, C., et al. (2025) Learning Care Pathways Framework: a new method to implement, learn, replicate, and scale up care pathways for and with the patient, International Journal of Health Policy and Management, 14, 8517. doi: 10.34172/ijhpm.8517
Health Services Safety Investigations Body (2023) Safety management systems: an introduction for healthcare. Available at https://www.hssib.org.uk/patient-safety-investigations/safety-management-systems/investigation-report/ (Accessed 8 April 2026).
Health Services Safety Investigations Body (2025a) Safety management: accountability across organisational boundaries. Available at https://www.hssib.org.uk/patient-safety-investigations/safety-management/investigation-report/ (Accessed 9 March 2026).
Health Services Safety Investigations Body (2025b) Patient safety issues associated with electronic patient record (EPR) systems – a thematic review. Available at https://www.hssib.org.uk/patient-safety-investigations/electronic-patient-record-epr-systems-thematic-review/investigation-report/ (Accessed 9 March 2026).
Health Services Safety Investigations Body (2025c) Investigating under the Patient Safety Incident Response Framework (PSIRF): sharing HSSIB learning for future development. Available at https://www.hssib.org.uk/patient-safety-investigations/investigating-under-the-patient-safety-incident-response-framework-psirf-sharing-hssib-learning-for-future-development/investigation-report/ (Accessed 9 March 2026).
Holden, R.J., Carayon, P., et al. (2013) SEIPS 2.0: a human factors framework for studying and improving the work of healthcare professionals and patients, Ergonomics, 56(11), pp. 1669–1686. doi: 10.1080/00140139.2013.838643
NHS England (2025a) Working together in 2025/26 to lay the foundations for reform. Available at https://www.england.nhs.uk/long-read/working-together-in-2025-26-to-lay-the-foundations-for-reform/ (Accessed 9 March 2026).
NHS England (2025b) Strategic commissioning framework. Available at https://www.england.nhs.uk/long-read/strategic-commissioning-framework/ (Accessed 9 March 2026).
NHS England (n.d.a) Civility and respect. Available at https://www.england.nhs.uk/supporting-our-nhs-people/health-and-wellbeing-programmes/civility-and-respect/ (Accessed 9 March 2026).
NHS England (n.d.b) Governance, patient safety and quality. Available at https://www.england.nhs.uk/mat-transformation/matrons-handbook/governance-patient-safety-and-quality/ (Accessed 9 March 2026).
Patient Safety Learning (2023) The elephant in the room: patient safety and integrated care systems. Available at https://www.patientsafetylearning.org/blog/the-elephant-in-the-room-patient-safety-and-integrated-care-systems (Accessed 9 March 2026).
du Sartz de Vigneulles, B., Lan, R., et al. (2025) Improving care pathways through evidence-based modelling strategies: a scoping review, Public Health, 244, 105751. doi: 10.1016/j.puhe.2025.105751
The Health Foundation (2017a) Some assembly required: implementing new models of care. Lessons from the new care models programme. Available at https://www.health.org.uk/sites/default/files/SomeAssemblyRequired.pdf (Accessed 9 March 2026).
The Health Foundation (2017b) Ten lessons for redesigning care pathways. Available at https://www.health.org.uk/features-and-opinion/features/ten-lessons-for-redesigning-care-pathways (Accessed 9 March 2026).
The Kings Fund (2025) Integrated care board cuts – what does it all mean? Available at https://www.kingsfund.org.uk/insight-and-analysis/blogs/icb-cuts-what-does-it-mean (Accessed 9 March 2026).