A note of acknowledgement
We would like to thank the healthcare staff who engaged with the investigation for sharing their experiences, and for their openness and willingness to support improvements in this area of care.
About this report
This report looks at electronic prescribing and medicines administration (ePMA), which are digital systems used to prescribe and record the medication: given to a patient, or due and not given to a patient. In particular it focuses on procurement of new ePMA functionality and/or upgrades of existing ePMA functionality and how patient safety learning related to ePMA is identified and shared across the healthcare system. The investigation explored this in the context of the national legislative, regulatory, standards and assurance mechanisms relating to the safe use of ePMA that were in place up to April 2026.
The report is intended for healthcare organisations, policymakers and the public to help improve patient safety in relation to the procurement of, and safety learning from, ePMA functionality in acute NHS hospitals.
While it focuses solely on ePMA procurement and safety learning in acute NHS hospital settings, the investigation’s findings may be applicable to other care settings and other digital health technologies.
Terms used in this report
This report notes the close similarity between the NHS definitions of ‘digital health technology’ and ‘health IT system’ which are contained is some standards documents (NHS England n.d.a; 2025a; NHS Innovation Service, n.d.). For consistency, the term digital health technology is used in this report. See section 7 for a detailed glossary of terminology used in this report.
Executive summary
Background
This report examines patient safety in relation to electronic prescribing and medicines administration (ePMA). ePMA is software used to prescribe medication and create a record of the medication: that has been given, or due and not given to a patient. Most people admitted to hospital will receive medication, and most acute hospital trusts in England have ePMA functionality in at least part of their organisations.
This report focuses on the procurement process used by acute hospital trusts to purchase new ePMA functionality and/or upgrade their existing ePMA functionality and how patient safety learning about ePMA is identified and shared across the healthcare system. It considers how legal, regulatory, standards and assurance functions apply in relation to ePMA safety.
The patient safety risk
ePMA functionality has been shown to reduce some medication errors. However, the current national mechanisms (legislation, regulation, standards and assurance) for ensuring patient safety in relation to ePMA functionality may not adequately provide staff and healthcare organisations with the assurance that risk and hazard identification process are robust and/or share learning associated with the use of ePMA in an acute hospital setting.
The investigation
The investigation explored how national organisations, manufacturers and NHS acute hospital trusts collaborate and identify opportunities for improving patient safety in relation to the use of ePMA. This is the fourth and final report published under the HSSIB investigation theme of medication related harm.
Findings
- There are no core national patient safety standards that inform either the design or procurement of ePMA. This can lead to unwarranted variation in functionality across and between ePMA, other electronic systems, and acute hospital trusts, which may pose challenges for staff when prescribing and administering medication.
- Current assurance mechanisms do not provide national oversight or enforcement of either manufacturer or healthcare provider compliance with legally mandated standards relating to digital clinical safety and interoperability of digital health technology.
- The safety risks associated with software such as ePMA are complex and may change rapidly. Legislation, regulation and standards may not keep up with the speed of technological change.
- Manufacturers must self-assess and report whether their ePMA is compliant with relevant standards for their products to be included on an NHS procurement framework.
- There is variation in the core safety standards identified by acute hospital trusts when procuring and contracting for ePMA functionality. This leads to trusts identifying safety requirements individually, with limited consistency in the approach taken across trusts.
- Reliance is placed on acute hospital trusts to determine whether ePMA manufacturers have interpreted the medical device regulations appropriately, and to assure themselves that the trust complies with relevant standards. Some trusts do not have the resources, skills and expertise to do this effectively.
- Digital safety and patient safety teams at local and national level may work in silos, with limited ability to share information or collaborate on ePMA-related decisions that impact on patient safety.
- There are challenges with identifying national safety learning relating to ePMA as this is not reliably captured, shared or identified through formal reporting routes. There is ongoing work to improve the NHS reporting system to capture digital-related patient safety incidents.
- There is a reliance on informal networks for sharing ePMA safety issues which means safety concerns may not always be shared with those who need to be aware.
- Some ePMA manufacturers, whose ePMA functionality is not registered as a medical device choose to apply equivalent governance and assurance measures as if it is a medical device. This is in addition to complying with the digital clinical safety standard (DCB0129).
- Acute hospital trusts face challenges prioritising and resourcing procurement decisions for ePMA functionality. This leads to challenges and patient safety issues when ePMA is implemented.
- Clinical safety officers (CSOs) may not be adequately resourced, meaning they have limited capacity to support in managing clinical risks associated with ePMA.
- There is variation in how the CSO responsibilities set out in the digital clinical standards are interpreted and implemented by trusts. NHS England is working on plans for a formal curriculum and potential accreditation to improve CSO skills and capabilities.
HSSIB makes the following safety recommendations
Safety recommendation R/2026/086:
HSSIB recommends that the Medicines and Healthcare products Regulatory Agency ensures that:
- routes for manufacturers and healthcare organisations to engage with them are clear and accessible
- it reviews and provides further guidance and clarification on when electronic prescribing and medicines administration (ePMA) software should be considered a medical device.
This will support how ePMA software can be appropriately classified and regulated to improve patient safety.
Safety recommendation R/2026/087:
HSSIB recommends that NHS England/Department of Health and Social Care establishes a national framework for core electronic prescribing and medicines administration (ePMA) safety. This will provide a clear set of minimum patient safety requirements, helping to reduce unwarranted variation in the safety of ePMA functionality.
Safety recommendation R/2026/088:
HSSIB recommends that NHS England/Department of Health and Social Care develops an external assurance framework for information standards notices relating to electronic prescribing and medicines administration (ePMA). This is to reduce unwarranted variation and improve patient safety through expert-led assurance processes.
Safety recommendation R/2026/089:
HSSIB recommends that NHS England/Department of Health and Social Care provides additional support to acute hospital trusts, in relation to:
- supporting healthcare providers to access digital clinical safety knowledge, capacity and capability
- integrating digital clinical safety and patient safety, including the associated terminology
- supporting robust assurance of whether electronic prescribing and medicines administration (ePMA) manufacturers comply with relevant standards in order to be considered for inclusion on an NHS procurement framework.
This will support effective decision making and oversight by acute hospital trusts and reduce unwarranted variation in the understanding of, and approach to, adopting ePMA.
Safety recommendation R/2026/090:
HSSIB recommends that the Care Quality Commission reviews the sector-level assessment frameworks it is developing to include assurance of ongoing compliance with the digital clinical safety standard (DCB0160) for electronic prescribing and medicines administration (ePMA) software. This will help to ensure oversight of ePMA functionality to improve patient safety.
HSSIB makes the following safety observations
Safety observation O/2026/086:
Commercial manufacturers can improve patient safety by applying the standards and expectations for a medical device when developing electronic prescribing and medicines administration (ePMA) functionality, to help provide further assurance to acute hospital trusts procuring or updating ePMA functionality.
Safety observation O/2026/087:
Commercial manufacturers and NHS organisations can improve patient safety by ensuring the sharing of safety learning about electronic prescribing and medicines administration (ePMA) functionality nationally via incident reporting systems and relevant safety forums.
Safety observation O/2026/088:
Commercial manufacturers and NHS organisations can improve patient safety by contributing to and engaging with ePRaSE (ePrescribing Risk and Safety Evaluation) processes to support ongoing improvement and optimisation of electronic prescribing and medicines administration (ePMA) functionality across the NHS.
Local-level learning
HSSIB investigations include local-level learning where this may help organisations and staff to identify and think about how to respond to specific patient safety concerns at the local level. HSSIB has identified local-level learning to help organisations consider and mitigate risks around procuring ePMA, identifying and sharing learning from patient safety issues once ePMA is in use.
Supporting safe procurement of electronic prescribing and medicines administration (ePMA) functionality
How does your organisation:
- access the relevant skills and expertise, including clinical informatics, available to the ePMA project team so that patient safety is considered in decisions to upgrade or get new ePMA functionality?
- ensure that you have understood the medication processes used in everyday work (rather than as described in policy and procedure) and how these may be affected by introduction or changes to ePMA software?
- identify requirements for an ePMA that accounts for the needs of different staff groups, patients, and settings in which it will be used?
- identify whether the system can perform the tasks needed to meet organisational requirements and meet expected national safety standards?
- identify whether ePMA functionality meets relevant mandatory patient safety standards, such as digital clinical safety standards and interoperability information standards notices?
- ensure that the ePMA safety requirements are met by your preferred supplier if your ePMA functionality is part of a wider digital software procurement and/or upgrade?
- identify which of your safety requirements involve the manufacturer doing additional work, so that these issues and the timescale for delivery can be included in the contract?
- ensure relevant information (for example the safety case and hazard log) is requested from manufacturers and scrutinised during the selection and procurement of systems?
- identify whether it might be beneficial for the staff involved in the ePMA project to complete national digital clinical safety training?
Supporting patient safety learning from ePMA when the system is in use
How does your organisation:
- ensure the executive team is aware of their responsibility for digital clinical safety?
- ensure that there is sufficient CSO resourcing?
- ensure that the documentation for the ePMA clinical safety standard DCB0160 is reviewed and updated as needed?
- ensure that patient safety and digital safety is integrated locally?
- involve the medical device safety officer if the ePMA functionality is a medical device?
- promote reporting of potential patient safety issues via the local risk management system and Yellow Card reporting system if ePMA software is a medical device (SaMD)?
- collate potential ePMA-related patient safety issues from a range of sources to ensure that potential issues are identified?
- escalate ePMA safety concerns to the manufacturer?
- understand how well your ePMA functionality is optimised?
1. Background and context
1.1 Introduction
This report focuses on improving the patient safety aspects of procurement and how safety related learning from electronic prescribing and medicines administration (ePMA) functionality in NHS acute hospitals is identified and shared across the healthcare system.
This section provides background and context relating to the legislative, regulatory, standards and assurance aspects of healthcare discussed in the investigation. A glossary is available at section 7 to help explain some of the terms used in this section and throughout the report.
1.2 Digital health technology – national context
1.2.1 Digitising the NHS has been a national policy priority for many years (Darzi, 2024; Department of Health and Social Care, 2018; 2022; 2024; NHS England, n.d.b; Wachter, 2016). However, achieving these digitisation ambitions has proven to be ‘complex and challenging’, taking longer than planned (The Health Foundation, 2025).
1.2.2 The ‘10 Year Health Plan for England: fit for the future’ describes the shift from ‘analogue to digital’ as a key priority and includes recommendations to bring NHS technology up to date (UK Government, 2025).
1.2.3 Safety needs to be built in at every stage of the lifecycle of digital health technologies (DHTs), from design and procurement through to use and ongoing maintenance of DHTs. This allows potential safety risks to be identified and the risks to be appropriately mitigated. However, because DHTs and how they are used continue to evolve, not all risks to patient safety will be known in advance, and effective mitigation may only become clear over time (Sujan and Habli, 2021).
1.2.4 A report by the Nuffield Trust (2019) highlighted ‘the role national bodies need to play in setting and enforcing key national standards, and the opportunity to harness the collective buying power of the NHS to make sure we get the products and services we need’.
Patient safety and digital clinical safety
1.2.5 The National Patient Safety Strategy describes how the NHS will improve patient safety (NHS England, n.d.c). The NHS digital clinical safety (DCS) strategy is an addendum to the patient safety strategy. It highlights the ‘huge potential to improve safety in health and care’ but warns that it is ‘essential that digital innovation is delivered safely and does not lead to unintended harms’ (NHS England, 2021).
1.2.6 The NHS DCS standards were made mandatory under section 250 of the Health and Social Care Act 2012. Put simply, DCS ‘is about making sure the technologies used in health and care are safe, and then using those technologies to improve patient safety’ (NHS England, 2021).
1.2.7 Patient safety incidents are ‘something unexpected or unintended has happened, or failed to happen, that could have or did lead to patient harm for one or more person(s) receiving healthcare’ (NHS England, 2026a). The Learn From Patient Safety Events service (LFPSE) is a national NHS system for the recording and analysis of patient safety events that occur in healthcare (NHS England, n.d.d). LFPSE uses a common taxonomy (classification system) for capturing reported safety incidents/events, including ‘any issue involving digital technology – software, hardware, infrastructure, data, automation, or AI if it impacts, or has the potential to impact, clinical decision making or the delivery of patient care’ (NHS England, 2026a). Staff can report patient safety events via their local risk management systems which are then shared with the LFPSE service. Use of LFPSE is mandated by the NHS Standard Contract for NHS trusts (NHS England, 2025b).
What is a standard?
1.2.8 NHS healthcare standards are intended to ensure quality, safety, and efficiency in patient care across England. They cover areas like patient safety, data sharing, and governance.
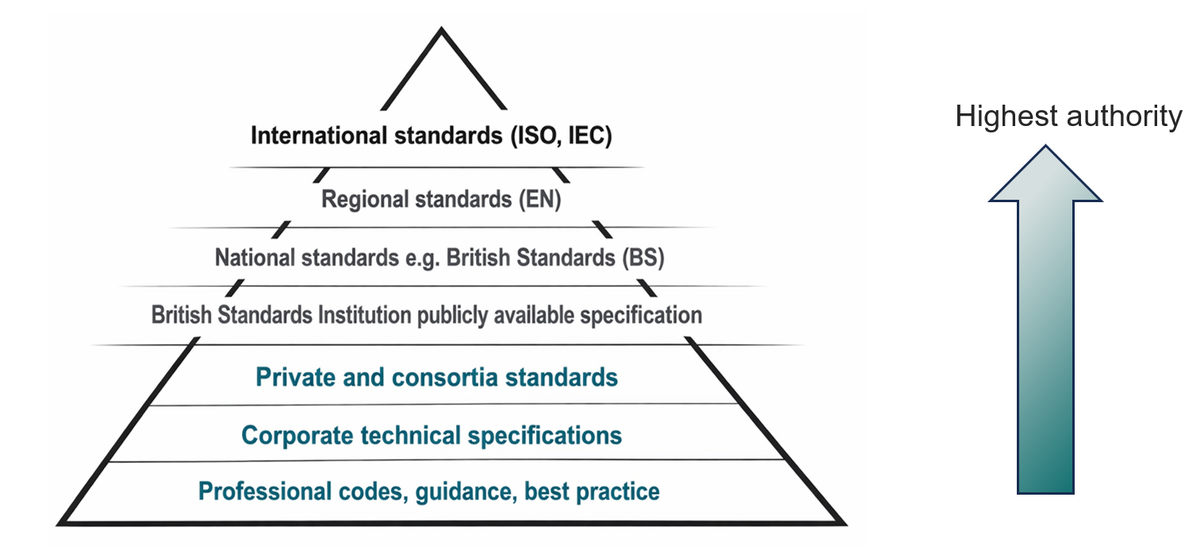
1.2.9 The International Organization for Standardization (ISO) (n.d.) defines a standard as ‘the distilled wisdom of people with expertise in their subject matter and who know the needs of the organizations they represent’. ISO suggests they be thought of ‘as a formula that describes the best way of doing something’.
1.2.10 There is no general requirement on how a standard is complied with. When conforming to a specific standard is mandatory, there is legislation describing who must conform with the standard.
1.2.11 Figure 1 shows where different guidance documents fit within a hierarchy of standards.
Figure 1 Hierarchy of standards (adapted from Chartered Institute of Ergonomics and Human Factors, 2023)
Patient safety standards, regulation and legislation
1.2.12 The investigation did not find and a widely used definition for a patient safety standard, so for this report used the following: the essential system requirements needed to prevent avoidable patient harm and manage clinical risk, ensuring safety is built into healthcare processes. The national standards that relate to patient safety and DHTs considered in this investigation report are summarised in this section.
NHS England standards
1.2.13 Information standards for health and care, which ‘define how data is collected, shared, and managed’ creating ‘a common language for health information’ (NHS England, 2025c). These standards are mandated for use in the NHS in England through information standards notices (ISNs), published under section 250 of the Health and Social Care Act 2012 (NHS England, 2025c).
1.2.14 The DCS standards which describe the clinical risk management process to evidence the safe development, deployment and use of DHTs are:
- DCB0129 for the health technology manufacturer (NHS England, 2025d)
- DCB0160 for the organisation deploying [implementing] and using health technologies (NHS England, 2023).
The DCS standards, published in 2018, are mandated under section 250 of the Health and Social Care Act 2012, are required under the NHS Standard Contract. A consultation on these standards was due to be launched during the investigation and was pending at publication.
1.2.15 The DCS standards describe the clinical risk management processes, which include a:
- hazard log – ‘a ‘key document’ that ‘underpins the work carried out to evaluate the clinical safety of a product… It describes the hazards, potential clinical impact of those hazards, mitigations and controls and final assessment of risk’
- clinical risk management plan
- clinical safety case ‘a structured argument which is supported by a body of relevant evidence that provides a compelling, comprehensible, and valid case that a system is safe for release’ (NHS England, 2025e)
- summary clinical safety case report.
1.2.16 The Digital Technology Assessment Criteria for health and social care (DTAC) is the ‘national baseline criteria’ for DHTs ‘entering and already used in the NHS and social care’ (NHS England, n.d.e). The DTAC has a broader scope than digital clinical safety, including interoperability, and usability and accessibility standards. This framework includes both good practice and legal requirements.
Medical device standards
1.2.17 Some functions performed by ePMA software may fall under the definition of a medical device, these include complex dose calculations for treatment and prevention of disease by warning about medication-to-medication interactions, in which case an additional requirement to those standards listed above must be met. Supporting guidance clarifies when a product is considered to be a medical device and how to decide if the manufacturer intends it to be used for a medical purpose (Medicines and Healthcare products Regulatory Agency, 2023a) (see 3.1). Manufacturers of systems that qualify as medical devices will need to take into account the safety of the whole system it is used in combination with.
Electronic prescribing and medicines administration
1.2.18 Electronic prescribing and medicines administration (ePMA) is defined as follows:
‘The utilisation of electronic systems to facilitate and enhance the communication of a prescription or medicine order, aiding the choice, administration and supply of a medicine through knowledge and decision support and providing a robust audit trail for the entire medicines use process.’ (NHS Connecting for Health, 2009)
In practical terms, an ePMA function in a hospital supports the safe, effective, and cost-effective use of medicines, from a patient’s arrival at hospital until their discharge.
1.2.19 There are many different types of ePMA functionality available in England, provided by a number of different software manufacturers. These can be bespoke (build in-house) or commercial off-the-shelf systems; standalone systems, or part of either an electronic medicines management system and/or digital healthcare record. The report considers all types of ePMA.
1.2.20 An ePMA research team funded by the National Institute for Health and Care Research (NIHR) developed the NHS ePrescribing toolkit (see figure 2) (ePrescribing Research Programme, n.d.a). This toolkit was commissioned by NHS England to support organisations planning to procure and implement ePMA functionality. It brings together learning and experience from trusts that have implemented ePMA, and been updated (NHS Futures, 2024). Some of the terms below are explained in the glossary.
Figure 2 Overview of the stages in the ePMA roadmap (adapted from the ePrescribing Research Programme’s toolkit)
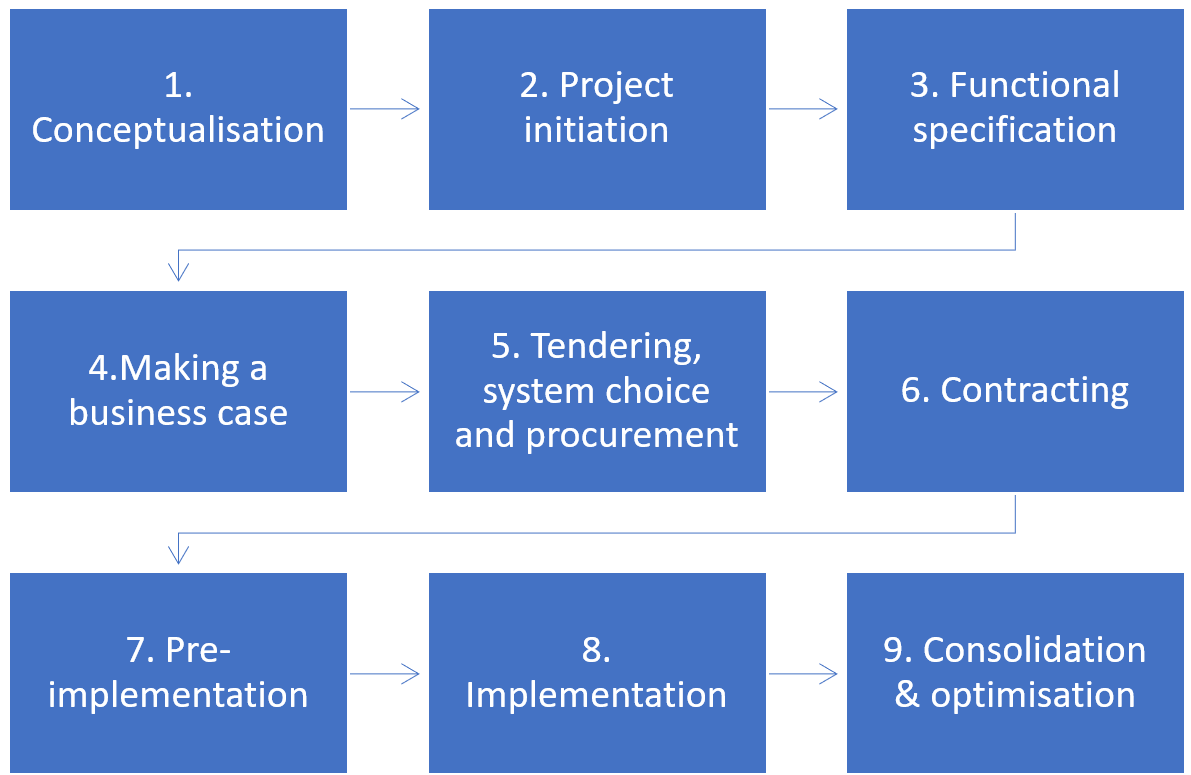
1.2.21 The investigation focused on the following stages of the ePMA roadmap:
- functional specification
- tendering, system choice and procurement
- contracting.
The investigation also considered how learning was shared about patient safety concerns when ePMA was in use (post contracting through pre-implementation to optimisation).
2. The patient safety risk
Electronic prescribing and medicines administration (ePMA) can help to reduce patient harm by preventing avoidable medication errors (Cattell et al, 2024). However, ePMA can also be associated with patient safety events and patient harm.
This section shares examples of risks and safety concerns related to ePMA that have been identified in previous Healthcare Safety Investigation Branch (HSIB) and HSSIB work. It also sets out wider national safety concerns that have been identified.
Previous investigations
2.1 A review of the 18 investigation reports by HSSIB, and its predecessor organisation HSIB, that included consideration of medication safety, was completed in 2024. Five out of 18 reports related to the use of ePMA (Health Services Safety Investigations Body, 2019; 2020; 2022a; 2022b; 2022c). Safety concerns related to ePMA configuration, use and interoperability with other health IT systems were identified that had the potential to cause harm if not recognised and managed. Some examples are given below.
Medication not given: administration of time critical medication in the emergency department
2.2 This investigation focused on a man with Parkinson’s who did not receive all of his Parkinson’s medication during a 3-day stay in the emergency department. As a result of the missed medications, he lost his ability to swallow and required feeding by a naso-gastric tube (a tube inserted into his stomach). The investigation found that the ePMA did not include a function to alert staff about patients who needed time critical medications to be prescribed or administered. The investigation also highlighted challenges in how staff had to adapt their practice to use the ePMA in some clinical environments, and the training and support in place for staff once the ePMA was deployed (Health Services Safety Investigations Body, 2024b).
Medication not given: anticoagulation before and after a procedure
2.3 An older man was admitted to hospital and his regular anticoagulant (medication that reduces the ability of a patient’s blood to clot) was temporarily paused as he had a nose bleed. The anticoagulant remained paused while he waited for a procedure. After the procedure, the anticoagulant was not restarted as intended. Two days after the procedure the patient had a stroke and died. The investigation found that there was no prompt within the ePMA to remind staff to review the paused anticoagulant and there was a delay to restarting the patient’s anticoagulant after the procedure. The investigation also highlighted how considerations about available equipment may affect the successful implementation of ePMA functionality (Health Services Safety Investigations Body, 2025a).
Medication not given: discharge from an acute hospital to the community
2.4 A man who had type 2 diabetes and used medications to manage his blood glucose levels was admitted to hospital and discharged home a week later. While he was in hospital the medication for managing his diabetes was changed and he was started on insulin. Seventeen days later it was identified that the man had not taken any insulin since he was discharged from hospital. He had high blood glucose and was admitted to hospital overnight for monitoring. The investigation found that there were multiple providers involved in the patient’s care; they used different ePMAs that did not interact to share information about his care (Health Services Safety Investigations Body, 2025b).
Electronic prescribing and medicines administration systems and safe discharge
2.5 Ann, a woman aged 75, took two anticoagulant medications at the same time, possibly causing an episode of gastrointestinal (digestive tract) bleeding. Ann was admitted to a hospice and died. One anticoagulant had been provided by the hospital when she was discharged home after a previous admission, and the other was a regular repeat supply provided by her community pharmacy. The investigation found that the hospital discharge summary did not interface with the ePMA and that the trust, primary care and community ePMA systems were not interoperable (Health Services Safety Investigations Body, 2019).
Weight-based medication errors in children
2.6 Felicity, a girl aged 4, received 10 times the intended dose of an anticoagulant medication on 5 occasions over one weekend. A subsequent scan showed she had a new bleed in the brain. The trust had made changes to their local ePMA configuration that was used for adult patients to allow its use for children. However, there was not a clear and consistent understanding of the potential hazards this introduced, meaning that adequate mitigation was not put in place. The investigation found gaps in local governance processes for ePMA functionality and digital clinical safety requirements (Health Services Safety Investigations Body, 2022b).
National patient safety concerns
2.7 The NHS Electronic Prescribing Risk and Safety Evaluation (ePRaSE) programme has found wide variation in how effectively ePMA functionality detects and prevents prescribing‑related harm across the NHS. Patient safety performance was strongly influenced by local configuration, optimisation, and ongoing maintenance, rather than by the manufacturers design of the ePMA functionality. This highlights the importance of local leadership and governance.
Different trusts using the same manufacturer’s ePMA showed markedly different abilities to mitigate prescribing risks, indicating that digital safety controls were not consistently implemented or sustained over time (Klein et al, 2025). The programme concluded that regular, structured testing of ePMA functionality is essential to identify latent digital safety risks and support continuous improvement (ePRaSE, n.d.a).
2.8 The Royal College of Paediatrics and Child Health (RCPCH) and Neonatal and Paediatric Pharmacy Group (NPPG) Medicines Committee have raised ongoing concerns about the safety of medication dosing with ePMA software in children. Specifically, ‘for frontline prescribers and the patients they treat, nothing has materially changed’ since the weigh-based medication errors in children report’s publication (see 2.6) and subsequent organisational responses. The committee describes this as ‘a systemic issue with EPMA adoption’ and calls a structured approach to integrate safety standards in paediatric EPMA; making recommendations on how this could be achieved (Bamber, 2026a; b).
2.9 A national patient safety alert was issued after incidents where penicillin allergies were incorrectly recorded as penicillamine allergies in ePMA, putting patients at risk of serious harm (NHS England, 2025f). This meant some patients with a penicillin allergy were prescribed penicillin‑based antibiotics, resulting in life‑threatening anaphylaxis and at least one reported death. The risk is increased by ePMA design features such as alphabetical listing of medication in drop‑down menus and allergy search results.
The alert required organisations to identify affected patients, correct allergy records, strengthen training, and work with digital health technology suppliers to reduce the risk of recurrence (NHS England, 2025f). It took time for this safety issue to be shared nationally, having previously been reported in 2019 by an acute hospital medication safety pharmacist (Willis, 2025).
Summary
2.10 The investigations and safety concerns set out above demonstrate examples of ePMA functionality and configuration impacting on patient safety once an ePMA has been implemented. However, HSSIB’s investigations have not explored in depth how ePMA are initially procured, or upgraded, to help ensure and improve patient safety.
2.11 The HSSIB investigation ‘Patient safety issues associated with EPR (electronic patient record) systems – a thematic review’ identified patient safety risks when ‘choosing an EPR system capable of meeting the needs of an organisation’ (Health Services Safety Investigations Body, 2025c). This consideration also applies to ePMA functionality.
2.12 This investigation considered there was an opportunity to explore whether problems reported at later stages of implementation could have been identified and mitigated had these been considered earlier on when procuring ePMA functionality. The investigation also considered how safety learning about ePMA functionality was shared, once an ePMA was being used, to influence future design, procurement decisions and ongoing optimisation.
3. Analysis and findings
The investigation explored the roles and responsibilities of key organisations involved in setting and regulating relevant patient safety standards. It also looked at how co-ordination and collaboration to improve the safety of electronic prescribing and medicines administration (ePMA) functionality could be achieved.
This section sets out the findings for each organisation in turn and describes the mechanisms for identifying and sharing learning about ePMA-related patient safety issues. The investigation used the foundations of System-Theoretic Accident Model and Processes (STAMP) and its tools (both STPA Hazard Analysis and CAST Accident Analysis) (see section 6/appendix) to map out organisations responsible for fulfilling safety constraints, and how they interact, make decisions and gain feedback about ePMA safety. Details of this approach are set out in the appendix and a high-level Control Safety Structure is shown at figure 3.
Figure 3 High-level overview of the main legislation, regulations and standards involved with ePMA procurement and safety learning
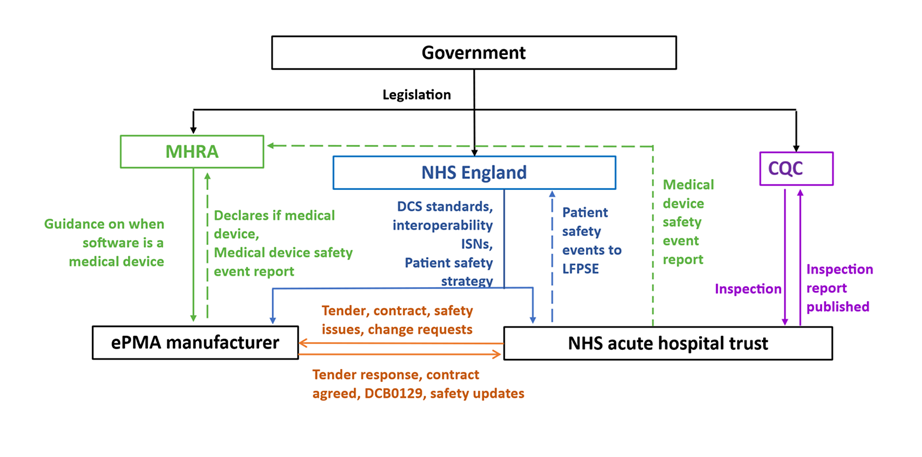
The investigation considered:
- the standards that ensure patient safety is included in ePMA design
- how an ePMA is procured
- how patient safety legal, regulatory and assurance functions operate in relation to ePMA
- how patient safety concerns and good practice are identified, addressed and shared to support improvements in the design of ePMA.
The investigation acknowledges that the digital healthcare space is rapidly evolving and that several of the national safety standards were under review during the investigation and at the time of publication. Therefore, the investigation’s findings relate to the landscape as it was up to April 2026.
3.1 Medicines and Healthcare products Regulatory Agency (MHRA)
Legislation
3.1.1 The MHRA ensures that medical devices meet the requirements set out in The Medical Device Regulations (2002) (MDR). For software, such as an ePMA, to qualify as a medical device it must have an element of autonomous clinical decision making built into the system. This is when a system has built-in decision-making tools that do not require human input, such as allergy checking against electronic patient records (EPRs). For software, such as an ePMA, to qualify as a medical device it must be intended to be used for a purpose listed in the definition of a medical device (Medicines and Healthcare products Regulatory Agency, 2026a).
3.1.2 MHRA does not regulate devices that are manufactured in-house, but it does provide guidance on best practice (Medicines and Healthcare products Regulatory Agency, 2026b). MHRA has recently published a call for evidence on a Health Institution Exemption for in-house manufacture and published the outcome (Medicines and Healthcare products Regulatory Agency, 2025). Healthcare organisations building their own systems or adapting commercial systems off label should follow MHRA's best practice guidance (Medicines and Healthcare products Regulatory Agency and Javid, 2021).
3.1.3 The MHRA told the investigation that many ePMAs may not meet the criteria for a medical device, as the ePMAs in themselves do not have the software functionality embedded into them that informs clinical decision making. For example, an ePMA may send requests to other EPR software (used for collecting, storing and managing data about individual patients), which is a medical device, for information such as allergy checking. The ePMA itself does not do this check, it just requests and receives information. The investigation found that this creates a safety gap as the ePMA is the system that is displaying critical information but has not undergone the rigors of medical device testing, assurance and MDR compliance.
3.1.4 The investigation spoke to several ePMA manufacturers who described that their systems were not a medical device. This meant they did not have to comply with the MDR. However, some manufacturers recognised that ePMA were so integrated with other EPRs that they had made a business decision to consider their ePMA as a medical device, but had not registered them with the MHRA as such. This ensured that the development and assurance processes they were using for ePMA were to the same standard as those for other medical devices that they produced.
3.1.5 The current criteria for whether a product is a medical device are set out in the MDR. The MHRA provides detailed guidance on the definition of a medical device and information to support decision making on whether a product is a medical device (Medicines and Healthcare products Regulatory Agency, 2023a;b). However, the responsibility for making this determination about specific products lies with the manufacturer of the product. The MHRA can provide advice on a case-by-case basis if asked (Medicines and Healthcare products Regulatory Agency, 2023b).
3.1.6 There is no external scrutiny from the MHRA or another regulator to make assessments where a product is being used that has not been assessed by the manufacturer as a medical device. For example, in the case of an ePMA, if a manufacturer decided that its software was not a medical device, it could market the software for use and there would be no external scrutiny, testing or assurance by a national regulating body. If the MHRA was aware of a breach, then they could take regulatory action.
3.1.7 Regardless of whether a product is assessed as being a medical device the manufacturer would still need to comply with the national digital safety standards, described in section 3.2. There is overlap between these standards and some hospital staff told the investigation that that this may not be consistently understood by manufacturers.
3.1.8 In 2022, HSIB recommended that the MHRA ‘works with the manufacturers of electronic prescribing and medicines administration systems to provide guidance on their obligations under the Medical Devices Regulations 2002 (as amended)’ (Health Services Safety Investigations Body, 2022b). In response to which the MHRA: contacted each ePMA manufacturer to review the regulatory status of their device, and took steps to improve reporting of potential errors with ePMA software to the MHRA (Medicines and Healthcare products Regulatory Agency, 2023c).
Safety learning
3.1.9 Whether an ePMA is classified as a medical device or not has an effect on the continuous monitoring of the product after it has gone to market. Only issues related to medical devices can be reported via the MHRA’s Yellow Card system (UK Government, n.d.). The investigation heard from NHS England, MHRA and manufacturers that if an ePMA was not considered a medical device this could inhibit the sharing of common concerns across different ePMA software, manufacturers and healthcare organisations. The MHRA told the investigation that it had not received any Yellow Card reports that relate to ePMA.
3.2 NHS England
Safety standards
3.2.1 The investigation found that there are no national patient safety standards that apply to the use of the majority of ePMA functionality. There are UK standards for the ‘safer use’ of ePMA for systemic (meaning throughout the body) anti-cancer treatment (UK Chemotherapy Board, 2022), but these do not apply outside of this specific area of care.
3.2.2 NHS England is responsible for maintaining the national digital clinical safety (DCS) standards and interoperability information standards notices (ISNs) (see 1.2.13 to 1.2.15) which apply to software, including ePMA. The investigation found that there is no feedback to NHS England on whether trusts are complying with the standards, and no enforcement action for non-compliance. Staff in an NHS trust told the investigation that this was in contrast to what happened if the trust did not meet other mandatory standards, such as for information governance.
3.2.3 Staff across the healthcare system felt frustrated because the DCS standards and ISNs were not well promoted or enforced nationally. This meant that the onus fell to trusts to ensure that ePMA manufacturers met these standards as part of their procurement and contracting processes.
3.2.4 Legislative changes enacted in July 2025 to section 250 of the Health and Care Act mean that current ISNs will not be valid after July 2027. NHS England told the investigation that it was in the process of agreeing which standards are the ‘building blocks of health and care systems’ and these would be given an ISN. Under the amended legislation, both trusts and ePMA manufacturers will be ‘required to comply’ with ISNs issued under this legislation. This will be reinforced under the Data (Use and Access) Act 2025, with its yet-to-be-published guidance (due late spring 2026). This will include the potential for penalties to be applied for non-compliance. However, the investigation was unable to gain clarity or understanding on how compliance may be monitored.
3.2.5 In its investigation report on weight-based medication errors in children, the Healthcare Safety Investigation Branch (HSIB) recommended that the NHS Digital and NHSX ‘promote the organisational requirements for digital clinical safety, including organisations’ responsibilities in terms of safety cases and clinical safety officers, to encompass system functionality and processes’ (Health Services Safety Investigations Body, 2022b). The investigation reflected on progress since this safety recommendation, following the integration of NHS Digital and NHSX into NHS England and found that there had been some progress, but that further support was needed to fully embed these responsibilities at trust level (see 3.6).
3.2.6 The DCS standards were under review at the time of this investigation, for which the investigation heard widespread support. The investigation heard that a key reason for this review was the change in the digital landscape, from big software releases with longer time periods in between to a “more agile approach with continuous deployment much faster, smaller, quicker”.
3.2.7 One aspect of the DCS standards that may cause confusion is that are referred interchangeably as safety standards and clinical risk management processes. There is well‑recognised confusion in healthcare between risk management and patient safety, with evidence that the two are often conflated in name but not function, limiting effective harm prevention (Napier and Youndberg, 2008). Some staff interviewed felt that patient safety was ensured by following the risk management process. Some staff suggested that using only risk management in their title and description would be preferable, as this was clear and unambiguous.
3.2.8 The investigation was told that there was confusion about the regulation of the DCS standards. Colleagues at NHS England thought this fell to the Care Quality Commission (CQC) as part of monitoring compliance with the NHS Standard Contract; they had reached out to get clarification from the CQC, but this remained unclear. The CQC’s position is explored in 3.3.
3.2.9 The investigation met with representatives from the NHS England clinical informatics team who clarified that the clinical safety officer (CSO) in an NHS acute trust is accountable for “articulating the risk”. This means describing the ePMA functionality, its scope, what the hazards are, what mitigations have been put in place and what the residual risk is. Typically, this work is led by the CSO with input from a wide range of staff including the staff who will use the ePMA. It is then for the trust executive team “to sign off [or not] whether to proceed with the product in its current state” (see 3.6). The investigation heard from some stakeholders that there are “grey area[s]” around the accountability of systems and risks between CSO and executive teams and that “hopefully something that gets clarified in the standards review/revision”.
3.2.10 NHS England was working on a shift from national CSO training to training via digital skills networks, with plans for a formal curriculum and potential accreditation to ensure ongoing competence. This could help provide a minimum level of digital clinical safety skills at organisational level to support compliance with the DCS standards.
3.2.11 This training is one part of the DCS training portfolio designed to progressively ‘grow skills and competence’, from essential up to practitioner level, to enable compliance with the DCS standards (NHS England, 2026b). Essential (level one) training provides a ‘basic introduction to digital clinical safety and supports a culture of digital clinical safety across the NHS’, suitable for ‘all staff’ working in healthcare or for digital healthcare technology manufacturers. NHS England suggested it would be useful if staff involved in an ePMA project completed the ‘essential’ training.
3.2.12 An NHS England clinical informatics representative said that it was eager to work more closely with the procurement team that produces the NHS clinical digital procurement framework, so manufacturers are required to demonstrate their compliance with the DCB0129 standard. This collaborative working would be essential as the clinical informatics teams provides specialist advice to the NHS procurement framework provider about technical aspects of compliance with the DCS standards and interoperability ISNs (see 3.5).
Safety learning
3.2.13 The investigation found there was variation in people’s understanding of the term digital clinical safety, which may in part have arisen because it was appended to the patient safety strategy. An NHS England representative explained that the term meant patient safety applied to digital processes, and emphasised the need to help people understand how digital systems affect patient safety. They described plans to include digital safety more clearly in the forthcoming patient safety strategy update. Representatives from the clinical informatics team described how they were working in a more aligned way with the patient safety team nationally, and that this shift needed to be mirrored across the country.
3.2.14 The investigation conducted a search of Learn From Patient Safety Events (LFPSE) data and identified 127 reports that attributed a patient safety incident specifically to use of ePMA (see section 6/appendix). However, the reports provided limited insight into the nature of these incidents and the how ePMA contributed to them. This was due to factors such as:
- many of the questions used to categorise an incident being left incomplete
- many of the free text responses being unclear about the presence or absence of contributory factors, and in some cases unclear even about the event that had occurred.
3.2.15 These problems may reflect an inherent limitation in relying on incident reporting. That is, the recorder may not recognise potential implications of the incident for ePMA safety at the time of reporting, and therefore may not include the relevant information in the report. Healthcare staff may not report safety events due to fear of blame or punishment and the perception that reporting will not lead to learning or meaningful change (Macrae, 2016; Pfeiffer et al, 2010). Furthermore, it is difficult to assure that all concerns are reported to LFPSE, unless the data is corroborated with other intelligence sources (such as healthcare providers’ ePMA hazard logs and ePMA helpdesk queries).
3.2.16 The investigation met with representatives from the NHS England patient safety team to understand how national safety concerns about ePMA were identified and actioned when needed. A representative said they do see reports implying ePMA is involved in the incident context, but the specific problem may not be explicit in the safety event report. However, the team explained that trusts are additionally able to draw insights from the LFPSE data reported at their own locations, as they are aware of the local context surrounding a given incident, including what ePMA software is in use.
3.2.17 To address known limitations with incident reporting taxonomy, a group in Northern Ireland are building on a tool for ‘real-time recording and categorisation of EPMA-related contributory factors to medication errors’ (Relihan and Kelly, 2025) to develop a regional taxonomy for ePMA-related incidents. They plan to share the taxonomy with the manufacturer specific ePMA medication safety officer network.
3.2.18 The investigation learned that the patient safety team reviewed other sources of safety information in addition the reported safety events, including NHS helpdesk and cybersecurity data. NHS England regional teams may also escalate issues to them directly or via monthly joint quality and safety meetings.
3.2.19 There are several mechanisms by which national safety concerns related to digital systems are shared including dissemination to CSO’s, posting on the NHS digital community of practice forum (NHS Futures platform) and via regional integrated care board colleagues. A staff member explained that safety concerns focused on a “specific topic” but that ePMA may be one of the contributory factors.
3.2.20 An NHS England representative explained that there was ongoing work to improve the LFPSE service, focusing on refining the taxonomy and enhancing data capture for digital-related incidents. This aims to better identify and address the role of digital products in safety events.
3.2.21 A colleague in the clinical informatics team described how the clinical informatics and patient safety teams were purposely working in a more aligned way at a national level, and that this shift needed to be mirrored across the country.
3.3 Care Quality Commission (CQC)
Regulation
3.3.1 The CQC told the investigation that its role is to assess a healthcare provider against its minimum requirements set out in the fundamental standards of care (Health and Social Care Act 2008 (Regulated Activities) Regulations 2014). The role of the CQC is not to inspect the quality of an ePMA itself, but to ensure that safe and effective medication management is taking place in an organisation in the broader context.
3.3.2 The investigation was told by staff at trust and national level that they believed it was the CQC’s role to include the DCS standards in its inspection framework. Both CQC representatives and hospital staff told the investigation that the CQC’s focus was on healthcare outcomes, such as whether a medication error occurred, and not the prior processes. This means that if no medication errors are reported where ePMA is identified as a contributory factor, the systems safety aspects of ePMA are not necessarily explored. The CQC told the investigation that it may be in a position to confirm if an organisation has an ePMA safety case, but would be unlikely to assess them given the technical skills required to do so.
3.3.3 Trust chief pharmacists reported variation in whether or not CQC inspectors asked if the trust complies with standard DCB0160 for its ePMA functionality. The CQC told the investigation that it did not enforce the DCS standards but could ask for evidence of them having been completed (see 3.3.2).
3.3.4 In 2022, HSIB recommended that the CQC ‘reviews whether a provider’s assurance of its compliance with the Clinical Risk Management standard [DCB0160] specific to electronic prescribing and medicines administration systems in healthcare, can form part of the CQC’s developing regulatory model’ (Health Services Safety Investigations Body, 2022b). The CQC was asked for an update on progress. It explained that plans for a single assessment framework were abandoned and new sector-level assessment frameworks were published in draft for feedback, with the feedback period closing on 12 June 2026. This provides an opportunity for the CQC to identify how it could consistently consider compliance with the DCS standard in its assessment framework, to reduce the variation experienced by providers.
HSSIB makes the following safety recommendation
Safety recommendation R/2026/090:
HSSIB recommends that the Care Quality Commission reviews the sector-level assessment frameworks it is developing to include assurance of ongoing compliance with the digital clinical safety standard (DCB0160) for electronic prescribing and medicines administration (ePMA) software. This will help to ensure oversight of ePMA functionality to improve patient safety.
3.4 Manufacturers
3.4.1 There are many manufacturers of ePMA software in use in the UK. Many of the larger or well-established manufacturers produce ePMA functionality as a standalone system and/or as a module of a wider EPR system.
3.4.2 When a manufacturer designs an ePMA it has to follow certain documentation and process requirements. These mostly relate to the DCS standard DCB0129. Contained in the standard is a requirement to manage risk, produce hazard logs and a safety case, which must be given to the healthcare organisation that is procuring the ePMA (NHS England, 2025d). The procuring healthcare organisation then uses the information provided to develop their own risks, hazard logs and safety cases based on how they configure their system.
3.4.3 Several healthcare organisations said that they might have received an initial hazard log and safety case but that they needed “suppliers to be proactive and forthcoming with DCBs. When [an] upgrade happens [manufacturers] won’t always offer the updated safety case, may just provide a release note [detailing changes] for the upgrade”.
3.4.4 The investigation heard from several manufacturers that they use a root cause analysis (RCA) method to assess safety concerns with their ePMA software during the development stage. A human factors and ergonomics professional told the investigation that RCA may not fully assess safety concerns because of the linear nature of the method and its inability to consider systems holistically. These concerns are also reflected in academic literature (Peerally et al, 2017) and the move away from RCA as part of the NHS England patient safety strategy.
3.4.5 Manufacturers told the investigation that they had designed their ePMA software to be configurable by healthcare organisations, some giving full configuration control and others limited configuration control. This means that healthcare organisations can adapt the ePMA from the baseline system as procured to meet their own organisational needs, such as altering workflows or system alerts for high-risk medications. Several manufacturers told the investigation that they only maintained responsibility for the safety of a system up to the point that the system was configured locally by a healthcare organisation. They said that after any configuration had been undertaken, the ownership of risk sat with the healthcare organisation. “There needs to be full transparency between the system supplier and the Trust on the extent of configurability of the system and the extent of the Trust's responsibilities”.
3.4.6 The investigation found that despite manufacturers designing ePMA software so that they could be configured locally, they did not take responsibility for the adaptations and configurations made. In other safety critical industries, where end users configure equipment or software to meet their individual needs, there are checks and balances in place. These include the manufacturer acting as a safety design authority, to ensure that new risks resulting from changes are identified and managed. In civil aviation, for example, the manufacturer retains design authority of all safety critical software used and must approve all software changes, including configuration of the software relating to safety (Civil Aviation Authority, 2024).
3.4.7 Several manufacturers told the investigation that healthcare organisations are moving towards single manufacturer integrated EPR and ePMA, rather than standalone ePMA. They said that while standalone systems work well, there are significant benefits of having single-sourced EPR and ePMA rather than trying to integrate an ePMA with a different EPR. Where standalone ePMA software is used there is a need to ensure information is transferred between systems, which can be costly and inefficient, and potentially increase the chance of a patient safety event.
3.5 NHS procurement framework provider
3.5.1 NHS providers are recommended to buy ePMA functionality via an NHS ‘clinical digital health solutions (CDHS)’ framework. If funding for the product has been agreed with NHS England then the trust is required to purchase the product using an NHS procurement framework. At the time of writing this report there were 21 commercial manufacturers of ePMA functionality available on the CDHS procurement framework.
3.5.2 Although the procurement framework provider is responsible for identifying which standards are on the framework for manufacturers to meet, they work closely with partner organisations who will advise on which standards to include. The relevant partner organisations for safety are the NHS England clinical informatics team and MHRA. It is important to note that there are no national standards specifically relating to the design of ePMA systems and the CDHS framework provider cannot include standards that do not exist nationally.
3.5.3 Manufacturers that are on the procurement framework have applied to be there and have declared that they meet the required standards. In the case of the safe use of ePMA, this means the product meets standard DCB0129. Additionally, it complies with the MDR, but only if the manufacturer has deemed the product to be a medical device.
3.5.4 A representative from the CDHS framework provider told the investigation that manufacturers self-assess themselves as meeting the relevant requirements to be eligible for inclusion on the procurement framework. The procurement framework does not assure the responses given, so the onus is on manufacturers to provide an accurate response. They are required to review their responses annually.
3.5.5 The investigation found there was as assumption that if a product was on the CDHS framework that meant that it was a good or safe product to use. However, the presence of a product on the procurement framework means it meets the minimum requirements, but these are not specific to ePMA functionality.
3.6 Acute hospital trusts
Procurement and contracting
3.6.1 The investigation found that there was over-reliance on trusts to determine whether ePMA manufacturers had interpreted the MDR appropriately and to assure themselves that they complied with the interoperability ISNs and DCS standards (see 1.2.13 to 1.2.15). However, this expertise was not consistently available in house and trusts needed support in this area.
3.6.2 The investigation heard that the selection and procurement of an ePMA was usually led by a temporary project team which was disbanded after was implemented. Although local governance processes involve senior level approval, there was a reliance on the project team though its wider engagement to have identified and included appropriate user needs, specifications and contracts. Clinical and digital staff described variable, but limited, involvement in the pre-implementation process stages. Commonly the ePMA project team was relied upon to oversee those stages up to and including contracting, and would seek clinical input as needed.
3.6.3 Staff said that the trust focus was on the processes that happen after the contract with the manufacturer was signed. There was less understanding of the earlier processes, both in terms of how long these took and their importance for choosing an ePMA that is safe and easy to use. Furthermore, the shift to integrated EPR and ePMA meant that any ePMA safety considerations may be ‘watered down’ due to the number of requirements. The investigation was told that cost was invariably the overriding consideration: “the only thing that mattered was the price”.
3.6.4 Organisations with experience of previous ePMA deployments said that they did not know what they needed the first time an ePMA was deployed. At times, issues that would best have been resolved before contracting were being addressed during implementation.
3.6.5 The investigation was told that some “manufacturers won't share pre signing of contracts due to 'confidentiality' or 'intellectual property' concerns”. At times the manufacturer has asked for a non-disclosure agreement in order to access documents, even after contracts have been signed. These challenges were “often left to local CSOs to try and overcome” and highlighted the need for “additional support from higher within the NHS/organisation”.
3.6.6 Trust staff described lots of duplication, with each organisation working out what ePMA functionality was needed, translating this into requirements and then seeing whether these could be met by manufacturers as part of the tender process. Staff said examples of other organisations’ documents were shared, but there was no consensus on the core components of new ePMA functionality or how best to describe their needs. Several staff said that a specification of core requirements was developed and published under NHS Connecting for Health, but this was no longer signposted on the NHS website.
3.6.7 The investigation found that there was variation in trusts’ digital maturity and understanding of how to define ePMA requirements. The investigation heard from some trusts that they started from the principle that they just wanted their paper-based medicines administration system to be transferred to an electronic format. Others told the investigation that they started from a position of what they wanted from a system for the future, while incorporating safety and usability.
3.6.8 ePMA manufacturers explained there was variability in the quantity and quality of questions relating to safety asked as part of the tendering process. These ranged from a few broad questions, to numerous, very specific detailed questions. One manufacturer said sometimes essential safety requirements, that it knew the trust would want, were not included. Several manufacturers described that trusts should do the following at the tendering stage, to address key factors that impact on the safe use of ePMA:
- consider the range of staff who would use the ePMA, their roles and clinical settings
- understand how prescribing and medicines administration tasks were actually carried out every day, rather than what was supposed to happen according to policies and procedures
- involve the range of clinical staff from different settings who would use the ePMA to understand their needs and input their safety requirements
- ensure that usability was considered.
3.6.9 One issue that all the manufacturers noted was how questions were asked in the tender process. They explained that sometimes it appeared that questions were “relatively formulaic”, a “sort of checklist type approach to understanding the standards”. This was a concern as it may sometimes give “false reassurance to the trust … that they’re getting what they think they’re getting”.
3.6.10 Several staff said that it was possible to purchase an ePMA that did not comply with interoperability ISNs, and they felt this should not be possible. Others said that the manufacturers may say that it is possible to meet a requirement, but then it was important to include timescales for when that would be achieved in their contract, otherwise the trust had no leverage.
3.6.11 The investigation heard that, given the length of time between ePMA procurement exercises, the trust staff involved in the procurement and contracting are unlikely to do this more than once, so will have limited expertise. To support trusts, a draft contract is available from the CDHS framework provider for trusts to use, or they can choose to buy this expertise from the CDHS framework provider.
3.6.12 During consultation a CSO commented that ‘even though ‘intelligent procurement’ is considered as part of DCB0160’, procurement teams may not support ensuring that compliance documents are present pre-procurement. The CSO explained that once the ePMA functionality “has been purchased, the healthcare organisations often find they then have no leverage with which to try and enforce compliance. This meant that intelligent procurement needed to be ‘promoted and enforced locally’, with acute trust senior leadership/executive level support”.
4 Safety learning to promote co-ordination and collaboration across national organisations, manufacturers and NHS trusts
This section summarises the findings from section 3. It also describes safety learning to support improvements in electronic prescribing and medicines administration (ePMA) procurement and learning at national and acute hospital trust level.
Legislation and regulation
4.1 The underpinning legislation, regulation and standards relevant to digital health technologies (DHTs), including ePMA were developed over a decade ago and might not have kept up to date with software advances. While legislation will always lag behind technology, the safety risks associated with software are complex. Manufacturers and trust staff said that ePMA software can change rapidly compared to a traditional medical device or simple software or IT systems developed many years ago (for example continuously updated compared with quarterly updates).
4.2 The Medicines and Healthcare products Regulatory Agency (MHRA) told the investigation that it had undertaken consultations on changes to the UK device regulations in 2021 (Medicines and Healthcare products Regulatory Agency and Javid), 2024 and 2026. Additionally, the MHRA said that ePMA may or may not be a medical device depending on its intended purpose. However, software including ePMA is increasingly complex and some manufacturers choose to consider their ePMA as a medical device.
4.3 The investigation asked the Care Quality Commission (CQC), MHRA and NHS England about feedback mechanisms to the Department of Health and Social Care to monitor when legislation may need updating. The CQC said they have feedback mechanisms in place with regards potential updates to the CQC legislation. None were described by the MHRA or NHS England, yet many of those interviewed highlighted that the underpinning legislation needed revising.
4.4 A lack of clarity about when ePMA functionality may be a medical device, and a move from some manufacturers to treat ePMA as a medical device even when they may not be, can create confusion for acute hospital trusts. This can impact on procurement decisions and the ability to share safety learning about ePMA. The MHRA said that manufacturers are able to contact them for advice on the qualification and classification using the routes available.
4.5 The investigation heard from healthcare organisations that if ePMA software were considered to be a medical device it would give them improved confidence and assurance regarding its safety and development due to the quality and assurance processes associated with medical devices. They said that there would be greater assurance of systems and confidence to users around the development and assessment of system safety.
HSSIB makes the following safety recommendation
Safety recommendation R/2026/086:
HSSIB recommends that the Medicines and Healthcare products Regulatory Agency ensures that:
- routes for manufacturers and healthcare organisations to engage with them are clear and accessible
- it reviews and provides further guidance and clarification on when electronic prescribing and medicines administration (ePMA) software should be considered a medical device.
This will support how ePMA software can be appropriately classified and regulated to improve patient safety.
HSSIB makes the following safety observation
Safety observation O/2026/086:
Commercial manufacturers can improve patient safety by applying the standards and expectations for a medical device when developing electronic prescribing and medication administration (ePMA) functionality to help provide further assurance to acute hospital trusts when procuring or updating ePMA functionality.
Support for acute hospital trusts
4.6 The investigation identified a wide range of standards, frameworks and guidance about digital safety, produced across decades, in many different places on the internet and NHS Futures platform. It was difficult to identify which standards and legislation were required because of the large amount of information and many cross-references to other webpages.
4.7 In addition, there were roadmaps for implementing EPRs as well as ePMA roadmaps, and these are not aligned in terms of function at each stage of the relevant roadmap (NHS Futures, 2024; 2025). NHS England told the investigation that both applied if ePMA functionality was part of a wider EPR implementation. This created confusion for NHS acute trusts making procurement decisions about ePMA.
4.8 There are legally mandated standards relating to digital clinical safety and interoperability of digital health technology (DHT). However, there is variation in compliance with the standards by acute hospitals trusts and there is no national oversight or enforcement of healthcare providers’ compliance.
4.9 Individual trusts are relied on to determine whether ePMA manufacturers have interpreted the medical device regulations appropriately and to assure themselves that manufacturers have complied with relevant standards. Some trusts do not have the resources, skills, and expertise to do this effectively. Staff described longstanding financial and workforce challenges which impacted on trusts’ ability to recruit staff with the necessary clinical and/or digital skills. It was also challenging to release clinical staff from their clinical duties to contribute to an ePMA project.
4.10 The investigation heard support for minimising unnecessary duplication wherever possible so that staff could focus on other tasks; currently “each organisation seems to have to reinvent the wheel”. Suggestions included a national draft hazard log for trusts to use as a starting point for their risk assessments and function specifications, which included the relevant patient safety alerts and Never Events framework.
4.11 A recurrent theme that arose was the impact of staff cuts and redundancies, especially in non-patient facing roles. This affected digital staff and staff in roles involved with the pre-implementation stage of ePMA procurement, where not resourcing and prioritising patient safety may lead to unintended consequences.
Additional support from national organisations may help to support NHS acute trusts in understanding and making decisions about ePMA, to reduce variation and support safe and effective ePMA procurement.
HSSIB makes the following safety recommendations
Safety recommendation R/2026/088:
HSSIB recommends that NHS England/Department of Health and Social Care develops an external assurance framework for information standards notices relating to electronic prescribing and medicines administration (ePMA). This is to reduce unwanted variation and improve patient safety through expert-led assurance processes.
Safety recommendation R/2026/089:
HSSIB recommends that NHS England/Department of Health and Social Care provides additional support to acute hospital trusts, in relation to:
- supporting healthcare providers’ to access digital clinical safety knowledge, capacity and capability
- integrating digital clinical safety and patient safety, including the associated terminology
- supporting robust assurance of whether electronic prescribing and medicines administration (ePMA) manufacturers comply with relevant standards in order to be considered for inclusion on an NHS procurement framework.
This will support effective decision making and oversight by acute hospital trusts and reduce unwarranted variation in the understanding of, and approach to, adopting ePMA.
4.12 Due to significant changes across NHS England and the Department of Health and Social Care, the resources in national teams responsible for regulation and standards that affect ePMA is uncertain. This comes at a time when ‘digital by default’ is promoted as a national priority; however, external resources are having to be sought to enable NHS England to meet the 10-Year Health Plan’s key digital requirements (Serle, 2026).
4.13 Staff commented that there were other enablers that were key to improving the safe use of ePMA that needed to happen in tandem with regulation, legislation, standards and assurance. These included a range of considerations that could be had by NHS acute trusts to help better procure and share learning about ePMA. Examples included embedding a learning culture, and seeing clinical and technical involvement as a “strategic enabler to both quality and safety within the organisation”. Many staff told the investigation that collaborative working between the trust and manufacturer was essential to improving patient safety.
4.14 HSSIB investigations include local-level learning where this may help organisations and staff to identify and think about how to respond to specific patient safety concerns at the local level. HSSIB has identified local-level learning to help organisations consider and mitigate risks around procuring ePMA, identifying and sharing learning from patient safety issues once it is in use.
Local-level learning
Supporting safe procurement of electronic prescribing and medicines administration (ePMA) functionality
How does your organisation:
- access the relevant skills and expertise, including clinical informatics, available to the ePMA project team so that patient safety is considered in decisions to upgrade or get new ePMA functionality?
- ensure that you have understood the medication processes used in everyday work (rather than as described in policy and procedure) and how these may be affected by introduction or changes to ePMA software?
- identify requirements for an ePMA that accounts for the needs of different staff groups, patients, and settings in which it will be used?
- identify whether the system can perform the tasks needed to meet organisational requirements and meet expected national safety standards?
- identify whether ePMA functionality meets relevant mandatory patient safety standards, such as digital clinical safety standards and interoperability information standards notices?
- ensure that the ePMA safety requirements are met by your preferred supplier if your ePMA functionality is part of a wider digital software procurement and/or upgrade?
- identify which of your safety requirements involve the manufacturer doing additional work, so that these issues and the timescale for delivery can be included in the contract?
- ensure relevant information (for example the safety case and hazard log) is requested from manufacturers and scrutinised during the selection and procurement of systems?
- identify whether it might be beneficial for the staff involved in the ePMA project to complete national digital clinical safety training?
Supporting patient safety learning from ePMA when the system is in use
How does your organisation:
- ensure the executive team is aware of their responsibility for digital clinical safety?
- ensure that there is sufficient CSO resourcing?
- ensure that the documentation for the ePMA clinical safety standard DCB0160 is reviewed and updated as needed?
- ensure that patient safety and digital safety is integrated locally?
- involve the medical device safety officer if the ePMA functionality is a medical device?
- promote reporting of potential patient safety issues via the local risk management system and Yellow Card reporting system if ePMA software is a medical device (SaMD)?
- collate potential ePMA-related patient safety issues from a range of sources to ensure that potential issues are identified?
- escalate ePMA safety concerns to the manufacturer?
- understand how well your ePMA functionality is optimised?
Standards for ePMA functionality
4.15 The investigation was told of differences of opinion in whether it would be helpful to have core national ePMA safety standards, given the wide array of standards already in place for DHT. This was because medication management is a safety critical task and the existing standards do not focus specifically on ePMA functionality. A standard would reduce duplication by each acute hospital trust and ensure core standardisation across trusts.
4.16 Several national bodies, manufacturers and healthcare organisations said that core national safety standards would have been useful while ePMA was in its infancy, but could constrain manufacturers who had spent time and resources developing their product for a global market. There were also concerns that overly stringent safety standards could mean that some commercial manufacturers may choose to withdraw their product from sale in England.
4.17 In contrast, others said national standards would be beneficial, providing a level of standardisation that would be helpful when organisations sought to procure ePMA functionality. The current flexibility in ePMA functionality meant that a large amount of local configuration was needed to build the product, and the time and resources necessary to do this were often underestimated. Some degree of national standardisation would mean this configuration could be done by the manufacturer, or at least make the pre-implementation processes less time and resource intensive.
4.18 The investigation was told that trusts were tending to opt for an EPR with integrated ePMA. In this situation, ePMA safety requirements were one of many wider considerations. Some staff felt that, with no national minimum safety standards for ePMA functionality, ePMA safety may not be prioritised in decision making as part of a larger project.
4.19 On balance there was support for having mandatory core national safety standards (see 1.2.12) for ePMA that could be applied across healthcare settings, with the option for organisations to add to these as needed. This would enable NHS procurement framework providers to require compliance with such a standard to be eligible for inclusion on the clinical digital health solutions procurement framework. The investigation was told that some settings have different requirements, such as newborn critical care and maternity, where it is important that their needs can be met. These requirements are ‘over and above normal ePMA functionality’ and may have to be locally agreed. One example of national safety standards is those developed for weight based doing for children with ePMA (see 2.8).
HSSIB makes the following safety recommendation
Safety recommendation R/2026/087:
HSSIB recommends that NHS England/Department of Health and Social Care establishes a national framework for core electronic prescribing and medicines administration (ePMA) safety. This will ensure that a clear set of minimum patient safety requirements are used, helping to reduce unwarranted variation in the safety of ePMA functionality.
Learning about ePMA functionality
4.20 The investigation found that the MHRA Yellow Card scheme (see 3.1.9) and Learn From Patient Safety Events (LFPSE) service (see 1.2.7) only partly meets the needs of a feedback system to identify patient safety concerns with ePMA. Manufacturers, NHS acute trusts, and national bodies relied on informal routes, such as ePMA user groups and professional networks, to share this information, meaning that safety learning is not consistently and reliably captured.
4.21 The investigation acknowledges the limitations with the current formal feedback mechanisms, such as Yellow Card reporting and organisational safety event reporting and input to LFPSE. Improved sharing of information and collaboration within and across healthcare staff, organisations and ePMA manufacturers can improve safety learning so that potential hazards can be reviewed and any risks managed.
4.22 Acute hospital trusts can use the ePRaSE (ePrescribing Risk and Safety Evaluation) tool to support their assessment of whether their ePMA is functioning as they would want. This aligns with a recommendation that HSIB made to NHSX (now part of NHS England) in 2019 to ‘consider making ePRaSE a mandatory annual reporting requirement for the assessment and assurance of electronic prescribing and medicines administration safety’ (Health Services Safety Investigations Body, 2019).
4.23 The ePRaSE team launched the Electronic Prescribing Learning Lab in March 2026. This ‘interactive learning resource developed to support digital and pharmacy teams to optimise their electronic prescribing systems’ (ePRaSE, n.d.b).
4.24 A number of people and organisations who commented on the draft of this report recommended using tools such as ePRaSE to “test whether the ePMA system, as configured locally, effectively supports safe prescribing and administration” in practice. NHS England digital staff commented at consultation that “Results from ePRaSE testing would provide objective evidence of whether key risks are being mitigated, identify variability between organisations using the same [ePMA] system, and inform targeted improvement where controls are weak. Repeat testing would be expected following significant configuration changes, workflow redesign or system upgrades, recognising that ePMA safety performance can change over time". Safety assurance is “based on demonstrated safety performance rather than supplier self‑declaration”.
HSSIB makes the following safety observations
Safety observation O/2026/087:
Commercial manufacturers and NHS organisations can improve patient safety by ensuring the sharing of safety learning about electronic prescribing and medication administration (ePMA) functionality nationally via incident reporting systems and relevant safety forums.
Safety observation O/2026/088:
Commercial manufacturers and NHS organisations can improve patient safety by contributing to and engaging with the ePRaSE (ePrescribing Risk and Safety Evaluation) processes to support ongoing improvement and optimisation of electronic prescribing and medicines administration (ePMA) functionality across the NHS.
5. References
Bamber, J. (2026a) Safe and effective dose management in electronic prescribing and medicines administration systems. Available at https://www.rcpch.ac.uk/resources/safe-effective-dose-management-electronic-prescribing-medicines-administration-systems (Accessed 11 May 2026).
Bamber, J. (2026b) Optimising electronic prescribing and medicine administration (ePMA) systems – patient safety spotlight. Available at https://www.rcpch.ac.uk/news-events/news/2026-04/optimising-electronic-prescribing-medicine-administration-epma-systems (Accessed 11 May 2026).
Cattell, M., Hyde, K., et al. (2024) Retrospective review of medication-related incidents at a major teaching hospital and the potential mitigation of these incidents with electronic prescribing and medicines administration, European Journal of Hospital Pharmacy, 31(4), pp. 295–300. Available at https://ejhp.bmj.com/content/31/4/295 (Accessed 30 March 2026).
Chartered Institute of Ergonomics and Human Factors (2023) Demystifying ergonomic standards. Available at https://www.youtube.com/watch?v=sQ0B0tKZXKE (Accessed 30 March 2026).
Civil Aviation Authority (2024) Unmanned aircraft system operations in UK airspace. CAP 722. Ninth edition amendment 2. Available at https://www.caa.co.uk/publication/download/21784 (Accessed 30 March 2026).
Darzi, A. (2024) Independent investigation of the NHS in England. Available at https://www.gov.uk/government/publications/independent-investigation-of-the-nhs-in-england (Accessed 30 March 2026).
Data (Use and Access) Act (2025) Available at https://www.legislation.gov.uk/ukpga/2025/18/contents (Accessed 30 March 2026).
Department of Health and Social Care (2018) The future of healthcare: our vision for digital, data and technology in health and care. Available at https://www.gov.uk/government/publications/the-future-of-healthcare-our-vision-for-digital-data-and-technology-in-health-and-care/the-future-of-healthcare-our-vision-for-digital-data-and-technology-in-health-and-care (Accessed 30 March 2026).
Department of Health and Social Care (2022) A plan for digital health and social care. Available at https://www.gov.uk/government/publications/a-plan-for-digital-health-and-social-care/a-plan-for-digital-health-and-social-care (Accessed 30 March 2026).
Department of Health and Social Care (2024) Medical technology strategy. Available at https://www.gov.uk/government/publications/medical-technology-strategy/medical-technology-strategy (Accessed 30 March 2026).
ePRaSE (n.d.a) About ePRaSE. Available at https://eprase.info/about/ (Accessed 11 May 2026).
ePRaSE (n.d.b) EP Learning Lab. Electronic Prescribing Risk and Safety Evaluation Programme. Available at https://eprase.info/lab/ (Accessed 11 May 2026).
ePrescribing Research Programme (n.d.a) ePrescribing Toolkit. Available at www.eprescribingtoolkit.com (Accessed 30 March 2026).
ePrescribing Research Programme (n.d.b) ePrescribing Toolkit: consolidation and optimisation Available at https://www.eprescribingtoolkit.com/planner/consolidation-and-optimisation/ (Accessed 30 March 2026).
ePrescribing Research Programme (n.d.c) ePrescribing Toolkit: pre-implementation. Available at https://www.eprescribingtoolkit.com/planner/pre-implementation/ (Accessed 30 March 2026).
Health and Social Care Act 2008 (Regulated Activities) Regulations 2014. Available at https://www.legislation.gov.uk/uksi/2014/2936/contents (Accessed 7 May 2026).
Health Services Safety Investigations Body (2019) Electronic prescribing and medicines administration systems and safe discharge (Originally published by the Healthcare Safety Investigation Branch). Available at https://www.hssib.org.uk/patient-safety-investigations/electronic-prescribing-and-medicines-administration-systems-and-safe-discharge/ (Accessed 30 March 2026).
Health Services Safety Investigations Body (2020) The role of clinical pharmacy services in helping to identify and reduce high-risk prescribing errors in hospital (Originally published by the Healthcare Safety Investigation Branch). Available at https://www.hssib.org.uk/patient-safety-investigations/the-role-of-clinical-pharmacy-services-in-helping-to-identify-and-reduce-high-risk-prescribing-errors-in-hospital/ (Accessed 30 March 2026).
Health Services Safety Investigations Body (2022a) The use of an appropriate flush fluid with arterial lines (Originally published by the Healthcare Safety Investigation Branch). Available at https://www.hssib.org.uk/patient-safety-investigations/the-use-of-an-appropriate-flush-fluid-with-arterial-lines/ (Accessed 30 March 2026).
Health Services Safety Investigations Body (2022b) Weight-based medication errors in children (Originally published by the Healthcare Safety Investigation Branch). Available at https://www.hssib.org.uk/patient-safety-investigations/weight-based-medication-errors-in-children/ (Accessed 30 March 2026).
Health Services Safety Investigations Body (2022c) Medicine omissions in learning disability secure units (Originally published by the Healthcare Safety Investigation Branch). Available at https://www.hssib.org.uk/patient-safety-investigations/medicine-omissions-in-learning-disability-secure-units/ (Accessed 30 March 2026).
Health Services Safety Investigations Body (2024a) Medication related harm. Available at https://www.hssib.org.uk/patient-safety-investigations/medication-related-harm/ (Accessed 30 March 2026).
Health Services Safety Investigations Body (2024b) Medication not given: administration of time critical medication in the emergency department. Available at https://www.hssib.org.uk/patient-safety-investigations/medication-related-harm/investigation-report/ (Accessed 30 March 2026).
Health Services Safety Investigations Body (2025a) Medication not given: anticoagulation before and after a procedure. Available at https://www.hssib.org.uk/patient-safety-investigations/medication-related-harm/second-investigation-report/ (Accessed 30 March 2026).
Health Services Safety Investigations Body (2025b) Medication not given: discharge from an acute hospital to the community. Available at https://www.hssib.org.uk/patient-safety-investigations/medication-related-harm/third-investigation-report/ (Accessed 30 March 2026).
Health Services Safety Investigations Body (2025c) Patient safety issues associated with electronic patient record (EPR) systems – a thematic review. Available at https://www.hssib.org.uk/patient-safety-investigations/electronic-patient-record-epr-systems-thematic-review/investigation-report/ (Accessed 30 March 2026).
International Organization for Standardization (n.d.) Standards. Available at https://www.iso.org/standards.html (Accessed 30 March 2026).
International Organization for Standardization (2021) Health informatics – Interoperability and integration reference architecture – Model and framework. ISO 23903:2021. Available at https://www.iso.org/obp/ui/#iso:std:iso:23903:ed-1:v2:en (Accessed 7 April 2026).
Jeeves, B., Mullen, S., et al. (2025) CSO Council white paper. Digital clinical safety in the UK, an open and informed position: supporting CSOs to foster a culture of compliance with standards. Available at https://digitalhealthnetworks.net/wp-content/uploads/2025/03/CSO-Council-White-Paper-Digital-Clinical-Safety-in-the-UK-March-2025.pdf (Accessed 30 March 2026).
Klein, S., Tsanas, A., et al. (2025) A simulation study to quantitatively assess the performance of electronic prescribing systems in English NHS hospital trusts, Scientific Reports, 15, 2120. doi: 10.1038/s41598-025-86112-w
Leveson, N.G. and Thomas, J.T. (2018) STPA handbook. Available at https://psas.scripts.mit.edu/home/get_file.php?name=STPA_Handbook.pdf (Accessed 30 March 2026).
Leveson, N. (2024) CAST handbook. A “systems thinking” approach to the investigation of healthcare adverse events. Available at https://psas.scripts.mit.edu/home/get_file10.php?name=CAST_Handbook_Healthcare.pdf (Accessed 30 March 2026).
Macrae, C. (2016) The problem with incident reporting, BMJ Quality & Safety, 25(2), pp. 71–75. doi: 10.1136/bmjqs-2015-004732
Medicines and Healthcare products Regulatory Agency and Javid, S. (2021) Consultation outcome: Consultation on the future regulation of medical devices in the United Kingdom. Available at https://www.gov.uk/government/consultations/consultation-on-the-future-regulation-of-medical-devices-in-the-united-kingdom (Accessed 12 May 2026).
Medicines and Healthcare products Regulatory Agency (2023a) Borderline products: classifying medical devices and risk. Available at https://www.gov.uk/guidance/borderline-products-how-to-tell-if-your-product-is-a-medical-device (Accessed 13 May 2026).
Medicines and Healthcare products Regulatory Agency (2023b) Guidance: medical device stand-alone software including apps (including IVDMDs). Available at https://assets.publishing.service.gov.uk/media/64a7d22d7a4c230013bba33c/Medical_device_stand-alone_software_including_apps__including_IVDMDs_.pdf (Accessed 30 March 2026).
Medicines and Healthcare products Regulatory Agency (2023c) Drug safety Update: Electronic Prescribing and Medicines Administration Systems: report adverse incidents on a Yellow Card. Available at https://www.gov.uk/drug-safety-update/electronic-prescribing-and-medicines-administration-systems-report-adverse-incidents-on-a-yellow-card (Accessed 13 May 2026).
Medicines and Healthcare products Regulatory Agency (2025) Health Institution Exemption – Stakeholder survey: Call for Evidence Analysis Summaries. Available at https://www.gov.uk/government/calls-for-evidence/health-institution-exemption-stakeholder-survey/outcome/health-institution-exemption-stakeholder-survey-call-for-evidence-analysis-summaries (Accessed 12 May 2026).
Medicines and Healthcare products Regulatory Agency (2026a) Health Institution Exemption for general medical devices. Available at https://www.gov.uk/government/publications/health-institution-exemption-for-general-medical-devices (Accessed 12 May 2026).
Medicines and Healthcare products Regulatory Agency (2026b) Regulating medical devices in the UK. Available at https://www.gov.uk/guidance/regulating-medical-devices-in-the-uk#requirements-for-those-manufacturing-and-supplying-devices-in-great-britain (Accessed 12 May 2026).
Napier, J. and Youndberg, B.J. (2008) ‘Risk management and patient safety: The synergy and the tension’. In: Youngberg, B.J. (ed.) Patient Safety Handbook. 2nd edn. Sudbury, MA: Jones and Bartlett Publishers, pp. 3–21.
NHS Connecting for Health (2009) Electronic prescribing in hospitals. Challenges and lessons learned. Available at https://webarchive.nationalarchives.gov.uk/ukgwa/20130502102046/http:/www.connectingforhealth.nhs.uk/systemsandservices/eprescribing/challenges/Final_report.pdf (Accessed 30 March 2026).
NHS England (n.d.a) Progress against digital clinical safety strategic commitments Available at https://www.england.nhs.uk/patient-safety/patient-safety-systems/digital-clinical-safety-strategy/progress/ (Accessed 30 March 2026).
NHS England (n.d.b) Online version of the NHS Long Term Plan. Chapter 5: Digitally-enabled care will go mainstream across the NHS. Available at https://webarchive.nationalarchives.gov.uk/ukgwa/20250506042209/https://www.longtermplan.nhs.uk/online-version/chapter-5-digitally-enabled-care-will-go-mainstream-across-the-nhs/ (Accessed 30 March 2026).
NHS England (n.d.c) The NHS Patient Safety Strategy. Available at https://www.england.nhs.uk/patient-safety/the-nhs-patient-safety-strategy/ (Accessed 30 March 2026).
NHS England (n.d.d) Learn from patient safety events (LFPSE) service. Available at https://www.england.nhs.uk/patient-safety/patient-safety-insight/learning-from-patient-safety-events/learn-from-patient-safety-events-service/ (Accessed 11 May 2026).
NHS England (n.d.e) Digital Technology Assessment Criteria (DTAC): guidance for buyers and suppliers. Available at https://transform.england.nhs.uk/key-tools-and-info/digital-technology-assessment-criteria-dtac/ (Accessed 11 May 2026).
NHS England (2021) Digital Clinical Safety Strategy. Available at https://transform.england.nhs.uk/key-tools-and-info/digital-clinical-safety-strategy/ (Accessed 30 March 2026).
NHS England (2023) DCB0160: Clinical risk management: its application in the deployment and use of health IT systems. Available at https://digital.nhs.uk/data-and-information/information-standards/governance/latest-activity/standards-and-collections/dcb0160-clinical-risk-management-its-application-in-the-deployment-and-use-of-health-it-systems/ (Accessed 30 March 2026).
NHS England (2024) Building healthcare software – acute, community and mental health care. Available at https://digital.nhs.uk/developer/guides-and-documentation/building-healthcare-software/acute-community-and-mental-health-care (Accessed 30 March 2026).
NHS England (2025a) Applicability of DCB0129 and DCB0160. Terms and definitions. Available at https://digital.nhs.uk/services/clinical-safety/applicability-of-dcb-0129-and-dcb-0160/terms-and-definitions#:~:text=81001%2D1:2021-,Health%20IT%20system,hardware%2C%20software%20or%20a%20combination (Accessed 30 March 2026).
NHS England (2025b) NHS Standard Contract 2025/26. Technical guidance. Available at https://www.england.nhs.uk/wp-content/uploads/2025/04/08-nhssc-2526-technical-guidance.pdf (Accessed 30 March 2026).
NHS England (2025c) Information standards for health and care. Available at https://digital.nhs.uk/data-and-information/information-standards (Accessed 30 March 2026).
NHS England (2025d) DCB0129: Clinical risk management: its application in the manufacture of health IT systems. Available at https://digital.nhs.uk/data-and-information/information-standards/governance/latest-activity/standards-and-collections/dcb0129-clinical-risk-management-its-application-in-the-manufacture-of-health-it-systems (Accessed 30 March 2026).
NHS England (2025e) Digital clinical safety assurance. Available at https://www.england.nhs.uk/long-read/digital-clinical-safety-assurance/#:~:text=Hazards%20are%20documented%20in%20the,system%20is%20safe%20for%20release (Accessed 30 March 2026).
NHS England (2025f) National patient safety alert – harm from incorrect recording of a penicillin allergy as a penicillamine allergy. Available at https://www.england.nhs.uk/long-read/national-patient-safety-alert-harm-from-incorrect-recording-of-a-penicillin-allergy-as-a-penicillamine-allergy/ (Accessed 30 March 2026).
NHS England (2026a) Record a patient safety event. Available at https://www.england.nhs.uk/long-read/policy-guidance-on-recording-patient-safety-events-and-levels-of-harm/ (Accessed 11 May 2026).
NHS England (2026b) Digital clinical safety training. Available at https://digital.nhs.uk/services/clinical-safety/clinical-risk-management-training (Accessed 30 March 2026).
NHS Futures (2024) ePMA resource roadmap v2. Available at https://future.nhs.uk/EPRSupportHub/viewdocument?docid=197998885 (Accessed 30 March 2026).
NHS Futures (2025) EPR programme roadmap v1.71. Available at https://future.nhs.uk/connect.ti/EPRSupportHub/view?objectid=154241093 (Accessed 30 March 2026).
NHS Innovation Service (n.d.) Regulation. Digital healthcare technologies Available at https://innovation.nhs.uk/innovation-guides/regulation/digital-product-or-service/ (Accessed 30 March 2026).
NHS Learning Hub (2021) An introduction to clinical informatics. Available at https://learninghub.nhs.uk/resource/5983 (Accessed 30 March 2026).
Nuffield Trust (2019) Achieving a digital NHS. Lessons for national policy from the acute sector. Available at https://www.nuffieldtrust.org.uk/sites/default/files/2019-05/digital-report-br1902-final.pdf (Accessed 30 March 2026).
Oskrochi, Y., Roy-Highley, E., et al. (2025) Digital health technology compliance with clinical safety standards in the National Health Service in England: national cross-sectional study, Journal of Medical Internet Research, 27, e80076. doi: 10.2196/80076
Peerally, M.F., Carr, S., et al. (2017) The problem with root cause analysis, BMJ Quality & Safety, 26(5), pp. 417–422. doi: 10.1136/bmjqs-2016-005511
Pfeiffer, Y., Manser, T., et al. (2010) Conceptualising barriers to incident reporting: a psychological framework, Quality and Safety in Health Care, 19, e60. doi: 10.1136/qshc.2008.030445
Relihan, E.C. and Kelly, S.M. (2025) EPMA-related contributory factors to medication errors: development of a taxonomy to inform the optimisation strategy for an electronic patient record. International Journal of Medical Informatics 203. doi: org/10.1016/j.ijmedinf.2025.105990
Serle, J. (2026) NHSE seeks external digital support as job cuts continue. Available at https://www.hsj.co.uk/finance-and-efficiency/nhse-seeks-external-digital-support-as-job-cuts-continue/7041117.article (Accessed 30 March 2026).
Sujan, M. and Habli, I. (2021) Safety cases for digital health innovations: can they work?, BMJ Quality & Safety, 30, pp. 1047–1050. doi: 10.1136/bmjqs-2021-012983
The Health Foundation (2025) Digitising the NHS and adult social care. What could it cost? Available at https://www.health.org.uk/reports-and-analysis/analysis/digitising-the-nhs-and-adult-social-care-what-could-it-cost (Accessed 30 March 2026).
The Medical Devices Regulations (2002) Available at https://www.legislation.gov.uk/uksi/2002/618/contents (Accessed 30 March 2026).
UK Chemotherapy Board (2022) Standards for the safer use of electronic prescribing and medicines administration (ePMA) systems for use in systemic anti-cancer therapy (SACT) services. Available at https://www.uksactboard.org/_files/ugd/638ee8_5613776913e5415f81f31610e4a4a862.pdf?index=true (Accessed 30 March 2026).
UK Government (n.d.) Report a problem with a medicine or medical device. Available at https://www.gov.uk/report-problem-medicine-medical-device (Accessed 30 March 2026).
UK Government (2025) Fit for the future – 10 Year Health Plan for England. Available at https://assets.publishing.service.gov.uk/media/6888a0b1a11f859994409147/fit-for-the-future-10-year-health-plan-for-england.pdf (Accessed 12 January 2026).
Watcher, R.M. (2016) Making IT work: harnessing the power of health information technology to improve care in England. Report of the National Advisory Group on Health Information Technology in England. Available at https://assets.publishing.service.gov.uk/media/5a8091afe5274a2e87dba8f2/Wachter_Review_Accessible.pdf (Accessed 30 March 2026).
Willis, S. (2025) Patient safety alert issued after penicillin allergies incorrectly recorded, The Pharmaceutical Journal, 315(8003). doi: 10.1211/PJ.2025.1.386805
6. Appendix
Investigation approach
This investigation explored how risks and safety concerns associated with electronic prescribing and medication administration (ePMA) are identified and acted upon at a national level.
The investigation was carried out between May 2025 and March 2026. The investigation scope spanned the organisations and processes involved from conception of the need for new or upgraded ePMA functionality by an acute NHS hospital trust until a contract with a commercial software provider was signed (or equivalent stage if the trust manufactured their own ePMA functionality), and learning once ePMA was in use.
Out of scope was: ePMA training, configuration, non-safety related aspects, independent hospital providers, non-acute physical health hospital settings, pharmacy dispensing and stock control aspects, global standards, and informal mechanisms such as good practice guidance and professional networks.
The investigation used the foundations of System-Theoretic Accident Model and Processes (STAMP) and its tools (both STPA Hazard Analysis and CAST Accident Analysis) in the investigation (Leveson and Thomas, 2018; Leveson, 2024). STAMP is a way of understanding safety issues in complex systems by focusing on how safety constraints are fulfilled (or not) by the various stakeholders in a system, including people, organisations, hardware, software, data, the interactions among them, along with the concept of inadequate control. STAMP uses a Control Safety Structure Model (see figure 3 in the main report) to map out who or what is responsible for fulfilling safety constraints, and how they interact, make decisions and gain feedback.
Evidence gathering
The investigation visited six trusts (five in person and one virtually) and engaged with trust staff at all levels, including those in executive, managerial, contracting, digital, clinical and patient safety roles.
Two focus groups were held with ePMA manufacturers (one in person and one virtual) and two in-depth virtual interviews took place with another two manufacturers.
Further evidence was gathered from relevant local and national policies and guidance, legislation and literature.
The NHS England Learn From Patient Safety Events service was searched, covering the date range 1 October 2023 to 30 April 2025 (number of records = 540,646). The following two searches were used to identify relevant records:
- Any record that includes:
- “IT Systems or Software” in the InvolvedAgents or ITSystemsInvolvementFactors field, and
- either a medication-related process in the InvolvedProcess field or “Medications” in the InvolvedAgents field.
- Any record that includes the term “ePMA” in the Description field.
The number of records extracted was 1,837. These records were hand searched in order to identify incidents attributed directly to ePMA according to the details provided. The final sample comprised of 127 records.
Stakeholder engagement and consultation
The investigation engaged with stakeholders and subject matter advisors to gather evidence during the course of the investigation. This also enabled checking for factual accuracy and overall sense-checking. The stakeholders contributed to the development of the safety recommendations based on the evidence gathered and are shown below:
| Comparison site organisations | Staff | National organisations | Subject matter advisors |
|---|---|---|---|
| Six different NHS acute hospital trusts. Ranging in type of trust, size of patient catchment area, location, number of sites, digital maturity, size and ePMA supplier | 29 trust staff | Medicines and Healthcare products Regulatory Agency | Systems safety engineer/ STAMP, STPA and CAST consultant |
| Four ePMA software manufacturers (UK, European, USA based and an in-house build) | 8 staff from commercial manufacturers | Care Quality Commission | Medication safety pharmacist and ergonomist |
| 3 digital specialists | NHS England (digital clinical informatics, digital medicines, technology digital and data, and patient safety teams) | ||
| 3 researchers | NHS framework procurement provider | ||
| Healthcare Information and Management Systems Society | |||
| Patient Safety Learning | |||
| National Institute for Health and Care Excellence |
7. Glossary
| Term | Definitiion |
|---|---|
| Clinical informatics | ‘The knowledge, skills and tools that enable information to be collected, managed, used and shared to support the delivery of healthcare and to promote health and wellbeing.’ (NHS Learning Hub, 2021) |
| Contracting | The formal legal arrangements and processes by which goods and services are procured and the main way of managing performance, quality, and payment. In the context of this report, this refers to an acute hospital trust purchasing ePMA functionality from a commercial supplier. |
| Configuration | In this report, configuration refers to how an organisation takes a procured ePMA functionality and sets it up for specific use within its own context. |
| Design (of ePMA software system) | Design is the development of a concept and then creation of a product. In this report, design refers to the initial development and creation of an ePMA functionality by the manufacturer. |
| Digital clinical safety | This refers to ‘making sure the technologies used in health and care are safe, and then using those technologies to improve patient safety’ (NHS England, 2021). |
| Digital clinical safety assurance | The process by which health IT used by care professionals is assured as safe and meets the required national standards. Clinical safety assurance is, in essence, a clinical risk management activity (NHS England, 2025d). |
| Digital healthcare | The use of IT systems, data and other digital tools to support the delivery of healthcare and to support high-quality patient outcomes. |
| Digital health technologies (DHTs) |
‘DHTs are apps, software, artificial intelligence (AI) and digital platforms or services used for health or social care. Some DHTs are considered to be medical devices. Software is likely to be a medical device if it: - results in a diagnosis or prognosis - influences treatment and decision making, including calculating risk - is linked to a medical device or medicine (potentially as an accessory)’ (NHS Innovation Service, n.d.). |
| Digital maturity | The extent to which an organisation has embraced and implemented digital healthcare to support and improve care. |
| Electronic patient record (EPR) system | Software for collecting, storing and managing data about individual patients (NHS England, 2024). |
| Electronic prescribing and medicines administration (ePMA) | ‘The utilisation of electronic systems to facilitate and enhance the communication of a prescription or medicine order, aiding the choice, administration and supply of a medicine through knowledge and decision support and providing a robust audit trail for the entire medicines use process’ (NHS Connecting for Health, 2009). |
| Electronic Prescribing Risk and Safety Evaluation (ePRaSE) | ‘an NHS-led web-based self-assessment tool that helps trusts understand how well their electronic prescribing (EP) systems are configured and maintained to mitigate known prescribing risks’ (ePRaSE, n.d.). |
| Functionality | The features of an IT system, such as ePMA software, and its ability to enable users to achieve their goal. |
| Functional specification requirements | See ‘Requirements’. |
| Hardware | The physical parts of IT systems, such as servers, laptops, handheld devices and monitors. It also includes the supporting infrastructure, such as Wi-Fi. |
| Hazard log | A ‘formal document specified in DCB0129 and DCB0160 which describes all the hazards that have been considered attributable to the product. It describes the hazards, potential clinical impact of those hazards, mitigations and controls and final assessment of risk’ (NHS England, 2025d). |
| Implementation | The processes of putting a plan, such as for a new ePMA functionality, into place. In this report, these processes include launch and ongoing support, including reviewing the hazard log and reporting potential ePMA safety issues. |
| Interoperability | The ability of a system, such as ePMA software, to work with other systems without special effort (International Organization for Standardization, 2021). |
| IT systems | The computer systems, hardware, software and networks in an organisation. |
| Learn from Patient Safety Events (LFPSE) service | A national NHS system for recording and analysing patient safety events that occur in healthcare. |
| Optimisation | The stage that follows implementation and launch, where a new product or service is continually refined and developed to realise its full potential (ePrescribing Research Programme, n.d.b). |
| Patient safety incident | These are ‘any unintended or unexpected incidents which could have, or did, lead to harm for one or more patients receiving healthcare’ (NHS England, n.d.d). |
| Pre-implementation | The stage before the launch of new functionality such as ePMA that involves developing the implementation strategy, designing and testing the ePMA work processes, planning training, and planning and testing for technical aspects and reporting arrangements (ePrescribing Research Programme, n.d.c). In this report, it includes completion of the ePMA hazard log and safety case, and gaining approval to make the new functionality live. |
| Procurement | The process of identifying and acquiring goods and services from other sources, such as software manufacturers. |
| Requirements | An organisation’s (documented) description of what a software, such as an ePMA system, should do and what it needs to provide for users and organisations. |
| Safety case | This is ‘a structured argument which is supported by a body of relevant evidence that provides a compelling, comprehensible, and valid case that a system is safe for release’ (NHS England, 2025d). |
| Software | Components of IT systems including programs, procedures and routines that instruct hardware on how to run tasks. |
| Standards | A formula that sets out the best way of doing something, informed by the ‘distilled wisdom of people with expertise in their subject matter and who know the needs of the organizations they represent – people such as manufacturers, sellers, buyers, customers, trade associations, users or regulators’. Standards cover a wide range of activities and ‘could be about making a product, managing a process, delivering a service or supplying materials’(International Organization for Standardization, n.d.). |
| Tendering | A structured, competitive procurement process where the purchaser invites external companies to bid for contracts to provide goods, services, or works. |