About this report
HSSIB has modelled an approach to investigating patient safety events under the Patient Safety Incident Response Framework (PSIRF). This is to support NHS organisations and investigation staff to increase their learning about how to investigate under this framework and provide examples of how PSIRF tools and guidance can be used to improve investigations. This report differs from the usual HSSIB report template as it uses the PSIRF patient safety incident investigation template.
The report also contains learning relevant to healthcare organisations and staff on potential areas for safety improvement within mental healthcare, specifically community mental health services.
Before reading this report
This report considers the care of a service user who experienced mental health problems and includes discussion about self-harm and attempted suicide. Some readers may find the contents of this report distressing. Information about how to access mental health support can be found on the NHS website.
Introduction
HSSIB engaged with a wide range of stakeholders, including clinicians and national leads, to learn more about the issues surrounding learning from patient safety events in mental health settings and to identify areas where an investigation could focus to help improve patient safety.
Although suicide has been the focus of extensive national work, it has persisted as a safety risk. The themes from incidents and complaints have remained the same over time. Evidence from the intelligence gathered suggests that greater insight into the challenges faced at an organisational level when a service user has attempted suicide, or taken their life, would be helpful.
To support NHS organisations and local investigation staff, HSSIB identified an opportunity to model approaches to patient safety incidents investigations (PSIIs) under the NHS Patient Safety Incident Response Framework (PSIRF). Stakeholders told HSSIB that this would help to increase local learning and provide examples of how PSIRF tools can be used to improve investigations. HSSIB has also used this opportunity to identify learning that may help to improve how PSIRF can support staff in carrying out incident investigations.
This investigation has used the PSII report template and PSIRF tools to investigate an attempted suicide in the community mental health setting. Findings and areas for improvement are listed for the organisations that were involved in this incident. However, the learning may be relevant to other organisations.
Patient safety incident investigation (PSII) report Mental health: attempted suicide while under the care of community services
| Incident ID number: | I-034394 (HSSIB) |
|---|---|
| Date incident occurred: | 9 August 2025 |
| Report approved date: | 2 April 2026 |
| Approved by: | HSSIB |
Terms used in this report
This patient safety incident investigation involves a mental health trust that provides community mental health services (CMHS). To protect anonymity, it is not named. The investigation involves referral from the GP to the mental health trust’s single point of access and onwards referral to their community mental health team (CMHT). The service user that this investigation related to is not named and is referred to as the ‘Service User’ throughout the report.
Distribution list
| The Service User and his partner | Divisional clinical governance lead |
| Patient safety lead | Service manager |
| Associate director of patient safety | Senior nurse manager |
| Key worker | Divisional director of nursing and quality |
| Mental health practitioner x 2 | Divisional medical director |
| Psychiatrist | Divisional associate director of operations |
| Clinical lead | GP practice manager |
| Operational team lead x 3 | |
| Pharmacist | |
| Mental health nurse |
About patient safety incident investigations
Patient safety incident investigations (PSIIs) are undertaken to identify new opportunities for learning and improvement. PSIIs focus on improving healthcare systems; they do not look to blame individuals. Other organisations and investigation types consider issues such as criminality, culpability or cause of death. Including blame or trying to determine whether an incident was preventable within an investigation designed for learning can lead to a culture of fear, resulting in missed opportunities for improvement.
The key aim of a PSII is to provide a clear explanation of how an organisation’s systems and processes contributed to a patient safety incident. Recognising that mistakes are human, PSIIs examine ‘system factors’ such as the tools, technologies, environments, tasks and work processes involved. Findings from a PSII are then used to identify actions that will lead to improvements in the safety of the care patients receive.
PSIIs begin as soon as possible after the incident and are normally completed within 3 months. This timeframe may be extended with the agreement of those affected, including patients, families, carers and staff. HSSIB started this investigation in October 2025, and it was completed in February 2026. The Service User was asked whether they wanted to be involved in the investigation and asked again whether they wanted to see the draft report, but did not wish to do so. The draft report was shared with staff involved in the patient safety incident for comments and feedback before being finalised.
If a PSII finds significant risks that require immediate action to improve patient safety, this action will be taken as soon as possible. Some safety actions for system improvement may not follow until later, according to a safety improvement plan that is based on the findings from several investigations or other learning responses.
An NHS organisation’s investigation team follows the Duty of Candour and the Engaging and involving patients, families and staff after a patient safety guidance in their collaboration with those affected, to help them identify what happened and how this resulted in a patient safety incident. Investigators encourage human resources teams to follow the being fair tool in the minority of cases when staff may be referred to them.
PSIIs within NHS organisations are led by a senior lead investigator who is trained to conduct investigations for learning. The investigators follow the guidance set out in the Patient Safety Incident Response Framework and in the national patient safety incident response standards.
A note of acknowledgement
This investigation focused on the care of the ‘Service User’, who attempted to end his life in August 2025. We would like to thank the Service User for supporting the investigation to explore his care. The Service User chose not to share his experience of care directly with the investigation team and we have therefore used information from the Service User's healthcare records and discussions with staff to provide an account of his care.
We would also like to thank the healthcare staff who participated in the investigation and who were keen to discuss and support improvements that might help make care for service users safer in the future.
About the Service User
At the time of publication, the Service User is living at home and receiving support from community mental health services.
When the incident took place, he was 42 years old. His healthcare records describe someone whose children and family are important to him, and who enjoys watching television, and when he feels well, going fishing and walking his dogs.
The Service User had a complex mental health history and had previously been in contact with mental health services. He had a number of co-existing mental health conditions and was prescribed medication for psychosis, anxiety and depression. The Service User felt that an antipsychotic he was prescribed was no longer working, he was experiencing side effects and wanted to try an alternative.
At the time of the incident the Service User lived in a house in a socially deprived city area with his son, and was not employed. He was not sleeping well at night, was experiencing problems with relationships, a lack of support, and struggled to leave his house. He was drinking alcohol every day and sometimes took drugs. It was documented that the Service User found this helped him ‘to cope with his voices’.
Executive summary
Incident summary
On 19 September 2024, the Service User visited his GP and asked for a medication review as he no longer felt his medications were effective in managing his mental health. The GP suggested doing another review in a few weeks' time so that the Service User could see how he felt after taking his medications at the intended dose, which he had not been doing before. At the second review appointment, on 10 October 2024, the Service User said he was still experiencing mental health symptoms and wanted to try an alternative. The GP referred him to his local NHS mental health trust via the single point of access (SPA) service.
A face-to-face appointment was booked with the community mental health team (CMHT) on 14 November 2024 which the Service User did not attend. Over the following 4 months appointments were booked for the Service User which he did not attend. There were several re-referrals made back into the SPA service as the Service User still required a medication review and support.
On 5 March 2025 the Service User attended an in-person appointment with a CMHT mental health practitioner. After this, an appointment was booked for a medication review with a psychiatrist (mental health specialist doctor). Two appointments were booked for the Service User in April and May, but he did not attend. A welfare visit was attempted in June with no answer at the Service User’s home address. Following a telephone call to the Service User a further appointment was booked for July 2025. The Service User was allocated a key worker on 21 July 2025 and attended his appointment with the psychiatrist on 29 July 2025.
The Service User’s medications were changed, and tests were booked to monitor his physical health. On 9 August 2025 the Service User attempted to end his life. He spent several weeks in hospital before being discharged home. He continues to be under the care of community mental health services.
Summary of key findings
The investigation found that:
- The Service User’s attempt to end his life was not expected by the mental health staff supporting him.
- The change to his medication meant it was a potentially vulnerable time for the Service User's mental health. This was despite him having a safety plan for how to seek help if he felt overwhelmed and planned monitoring check-ins in line with local procedure.
- The Service User’s case was complex and challenging; his mental ill-health, drug and alcohol use are likely to have impacted on his ability to reason and make informed decisions. Therefore, sharing of information across and between healthcare services was important to facilitate personalised care planning.
- Limited sharing of, and lack of ready access to, information about the Service User and his past mental health history impacted on the CMHS’s ability to provide effective and timely care.
- The Service User needed a tailored approach with reasonable adjustments to maximise his engagement with mental health services; there was a delay in his needs being identified and acted on.
- There was limited understanding and awareness by some staff of whether mental health medication can be offered to service users with mental health issues and concurrent alcohol use.
- Staff worked in a service that was overstretched and they had to make decisions about managing service user needs, service demand, and risk and safety, within limited resources. The demand for CMHT services exceeded the available capacity, impacting both service users and staff.
- Staff did not have the dedicated time and space to process and deal with distress they encountered as part of their daily work caused by incidents of patient harm.
- There are challenges to delivering the national ambition to provide a community focused model of care, many of which the mental health trust has limited or no control over.
Summary of areas for improvement
The investigation identified four areas of improvement which the mental health trust could develop safety actions to address.
Area of improvement 1
Making information about service users easily available and accessible across providers to support effective initial engagement and decision making.
Area of improvement 2
Early exploration of adjustments that individual service users might need to engage in the triage and referral processes.
Area of improvement 3
Staff knowledge and insight into how community mental health services can support service users who may require prescription medication and who use drugs and/or alcohol.
Area of improvement 4
Organisational support for protected time, resources and assistance for staff to mitigate and respond to the distress and demands they experience in their role.
Background and context
What is alcohol use disorder?
Alcohol use disorder (AUD) is a term used to describe a ‘range of mental health problems associated with alcohol’ use (Alcohol Change UK, n.d.). AUD means someone has ongoing problems with their alcohol use. They may find it hard to cut down or stop, even when alcohol is hurting their health, relationships, or daily life. AUD can range from mild to severe, with symptoms increasing in line with severity (Mayo Clinic, 2022).
AUD is considered a brain disorder due to the lasting changes in brain chemistry caused by alcohol use. Even a mild disorder can escalate and lead to serious problems, so early intervention is important.
The link between alcohol and mental health is complicated, and each can make the other worse. As described by Alcohol Change UK (2025), alcohol use ‘can be both a cause and a consequence of mental health problems, with some using alcohol to self-medicate, creating a cycle which can be difficult to break’.
Psychosis
Psychosis is a mental health condition that causes a person to perceive or interpret things differently from those around them. It can be described as ‘losing contact with reality’. These experiences feel completely real to the person, even though they are not happening outside their mind. This might involve seeing or hearing things that other people cannot see or hear (hallucinations) and believing things that are not actually true (delusions). It may also involve confused (disordered) thinking and speaking (NHS, 2023a). These symptoms can be very distressing and may lead to changes in the way someone behaves. When a person experiences this group of symptoms, it is often called a psychotic episode.
Treatment for psychosis involves a combination of antipsychotic medication, psychological therapy such as counselling, and practical support for day‑to‑day activities and social needs (NHS, 2023b). Often these symptoms can be treated in the community. However, if a person’s psychotic episodes are severe, they may need to be admitted to a mental health hospital for treatment (NHS, 2023a). With treatment, a person’s psychotic symptoms may permanently disappear, come and go over time, or remain but can still be managed (National Institute for Health and Care Excellence, 2014). When a person has both a mental health condition and AUD, it is recommended both are actively treated (Taylor et al, 2026a).
People who have had psychosis are more likely to have drug or alcohol use problems, or both. Some people use these substances as a way of trying to cope with psychotic symptoms.
Self-harm and suicide
Self-harm is ‘any behaviour where someone causes harm to themselves, usually as a way to help cope with difficult or distressing thoughts and feelings’ (Mental Health Foundation, 2022). Self-harm can be connected to difficult experiences, whether they are happening now or happened in the past. Sometimes a person may not know exactly why they are self-harming.
There is evidence of a clear link between suicide or suicidal thoughts and people who have previously and/or are currently self-harming (NHS, 2023c). However, not everyone who self-harms want to end their life.
What are community mental health services?
Community mental health services (CMHS) ‘provide care to individuals who need more support with their mental health than can be provided in primary care [for example, their GP]’ or have complex mental health needs. They are designed to ‘meet the mental health, physical health and wider social needs of individuals through multidisciplinary teams, which can include psychologists, psychiatrists, nurses, occupational therapists, social workers, and peer support workers. This includes individuals employed through statutory NHS bodies, local authorities and Voluntary, Community, Faith, and Social Enterprise organisations (VCFSE)’ (Health and Social Care Committee, 2025).
The investigation focused on several teams supporting adult service users within a CMHS including the:
- single point of access service
- adult community mental health team
- community social inclusion team.
The role of mental health practitioner (MHP) evolved to support those with severe mental illnesses, such as psychosis, to live well in their communities. The MHP role is based in GP practices or neighbourhood settings and can be taken on by a wide range of staff with mental health expertise (NHS England, n.d.).
Single point of access (SPA) service
This service is the ‘front door’ for local mental health services, open to both professionals and/or the public. The SPA service provides 24-hour access to mental health advice, and where necessary assessment, in a timely way according to the urgency of the situation. Referrals are wide ranging, from people experiencing a mental health crisis (when a person’s mental or emotional state quickly gets worse), to GPs seeking specialist input for one of their patients. The service does not cover immediate, life-threatening emergencies; these are referred to ‘999’ or the local emergency department.
When the SPA service receives a referral for a person who may need ongoing mental health support, an MHP will carry out a telephone triage. This involves the MHP asking the person questions to assess their current situation, exacerbating factors and the impact on their mental health. Following this screening process the MHP may signpost the person to appropriate support or refer them to one or more of the CMHS teams.
Adult community mental health team (CMHT)
Like the CMHS, the CMHT is diverse, including registered mental health nurses, social workers, psychiatrists, psychologists, occupational therapists and administrative staff. This multidisciplinary team (MDT) offers time-limited mental health treatment, care and monitoring for adults with complex and enduring mental health needs who can benefit from specialist support. This approach aims to provide holistic, person-centred care.
When someone is referred to the CMHT, they have a detailed in-person assessment which is carried out by an MHP. If the referral is appropriate for the CMHT then the person should be allocated a named MHP as a key worker, who acts as care planner and co-ordinator for a number of service users.
Treatment with medication
Antipsychotic medication works by blocking the effect of chemicals that transmit messages in the brain to help reduce psychotic symptoms (NHS, 2023b). The aim of medication treatment is to reduce and control psychotic symptoms while keeping side-effects at a minimum. Some people find a particular antipsychotic works better for them, causes fewer side effects or causes side effects that are easier to deal with. Those who are prescribed antipsychotics need additional physical health monitoring including for metabolic, hormonal and cardiovascular (heart and blood vessels) effects.
National guidance is available on the choice and monitoring of antipsychotic medication (National Institute for Health and Care Excellence, 2014). This guidance highlights the importance of:
- considering the effectiveness and side effects of the service user's current and previous medication, and
- monitoring for signs of improvement as well as side effects when a new antipsychotic is first started.
Antidepressant medication works by increasing levels of chemicals in the brain that are linked to mood and emotion. Antidepressants are used to treat the symptoms of depression, and some are also used for other conditions such as anxiety (NHS, 2025a). One type of antidepressant (selective serotonin re-uptake inhibitors or SSRIs) is usually the first choice because the side effects of SSRIs are generally easier to manage, and they are less likely to cause serious problems if taken in overdose (Taylor et al, 2026b).
Prescribed medication and alcohol
Interactions between alcohol and/or illicit drugs and prescribed medication for mental ill-health are common. National guidance recommends discussing with the service user the possible interference with the therapeutic effects of antipsychotics by other substances including alcohol and ‘illicit drugs’ (National Institute for Health and Care Excellence, 2014). It is not recommended to mix alcohol with an antipsychotic as this could increase the risk of side effects such as sedation, drowsiness, dizziness or falls (Anderson, 2025).
The Service User’s experience
September 2024 to December 2024
During a GP consultation on 19 September 2024, the Service User asked for a medication review as he no longer felt his medications were effective in managing his mental health. The GP identified that the Service User had been underdosing on the medication for his psychosis. It was agreed that the GP would review the Service User’s medication again after he had taken the intended dose for several weeks. The second review happened on 10 October 2024; the Service User said he still had mental health symptoms and wanted to try an alternative medication. The GP explained that he would need to refer him to the local mental health trust for this and confirmed that the Service User had contact details for emergency mental health support in the interim. The GP referred the Service User to the single point of access (SPA) service on 15 October 2024.
In response to the GP referral, on 21 October 2024 the Service User had a telephone triage appointment with a mental health practitioner (MHP). The Service User was discussed at the SPA multidisciplinary team (MDT) meeting with a psychiatrist. He was then referred to his local community mental health team (CMHT) for a medication review and told that ‘the next available appointment’ would be sent.
It was documented in the Service User’s healthcare records on 27 October 2024 that his partner, contacted the SPA service. She said the Service User had not taken medication for 5 days and was awaiting a medication delivery but was unsure who was arranging this. The Service User was present during the telephone call and when asked, confirmed he had no thoughts of harming himself or others at this time. During the telephone call, an in-person appointment was made with the CMHT for 14 November 2024. A text message was sent to the Service User’s mobile phone with details of the appointment.
The Service User did not attend the appointment on 14 November 2024. The healthcare records showed that his partner called the SPA service to ask for the Service User’s appointment to be rescheduled. She said that he had missed the appointment because he was asleep due to his medication. The appointment was rebooked for 3 December 2024. During the telephone call, it was documented that the Service User’s partner asked for the Service User’s mobile phone number be updated, which was done.
The Service User did not attend the appointment on 3 December 2024. It was documented that a telephone call was made by the MHP and his partner answered. She said the Service User was not there and had forgotten his appointment. She was advised that the Service User would need to make contact with the SPA service to be re-referred and that he had been discharged from CMHT.
On 5 December 2024 a CMHT staff member emailed the SPA service advising that the Service User had not attended and requesting that if he was re-referred, to remind the Service User of the importance of attending. On 9 December 2024 the SPA attempted to reach the Service User twice by telephone to try and rebook his appointment. Because the telephone calls were not answered he was discharged from the SPA service due to ‘lack of engagement’.
The following week, on 16 December 2024, the pharmacist at the Service User’s GP practice telephoned the SPA to rebook the Service User’s mental health medication review. The pharmacist advised that when the Service User took the intended dose of his medication for psychosis, this was associated with a ‘worsening in his claustrophobia and voices in his head’; therefore, he was to continue on the lower dose that he had been taking before September 2024. The pharmacist also said that as the Service User’s mental health was poor he did ‘still need to see CMHT’. In addition, the Service User had missed his CMHT assessment appointment due to poor mental health and now only had enough medication to last 7 days. The next available appointment with CMHT was booked for 17 January 2025.
January 2025 to August 2025
A CMHT MHP tried to telephone the Service User’s to remind him of his in-person appointment on 17 January 2025. The call ‘rang out’ and there was not a voicemail function available. The Service User did not attend his appointment on 17 January 2025. After this, the MHP made contact with the Service User’s nominated contact person, who said they had not seen or heard from the Service User. The contact person was updated on the situation and asked to inform the Service User that he had been discharged from the CMHT and that if he needed further medication, he should contact his GP or contact the SPA service to be re-referred.
On 19 January 2025, the SPA service sent the Service User a letter to say they had been unsuccessful in attempting to contact him and if he would like to speak to someone, he should make contact. On 22 January 2025 the Service User contacted the SPA service and apologised for not attending, stating he was unaware of the appointment. He asked for the referral to be re-opened and was set up on the system to receive appointment reminders by text message to his mobile phone.
The referral was re-opened on 27 January 2025 and a triage telephone appointment was booked with the Service User and took place on 9 February 2025. The outcome was to book an appointment with the CMHT for further assessment and a medication review. An in-person assessment with an MHP was booked and the Service User attended on 5 March 2025. During this appointment the Service User and the MHP agreed a care plan and a safety plan. The MHP offered to refer the Service User to a local partner organisation for alcohol support which he declined. The Service User said that he felt socially isolated and was given information about the community social inclusion team. He was told that after reading the information, the CMHT could refer him or he could self-refer. The Service User’s case was subsequently discussed at the CMHT MDT review meeting where it was agreed that he needed an appointment with a psychiatrist for a medication review.
An outpatient appointment was booked for 22 April 2025 with the psychiatrist and a letter was sent to the Service User confirming this. The Service User did not attend this appointment. The CMHT ‘duty worker’ telephoned the Service User, who apologised and reported ‘he overslept’. He said he would still like a medication review and an appointment was booked for 19 May 2025. The Service User said he was feeling slightly better as he had re-started some medications and reported no current concerns.
The Service User did not attend his rescheduled medication review outpatient appointment with the psychiatrist on 19 May 2025. He was sent an ‘opt-in’ letter should he still wish to use the mental health services. On 5 June 2025, an MHP visited the Service User’s house to see how he was, but there was no answer. The MHP telephoned the Service User who said he still wanted a medication review. When the missed appointments were raised, the Service User said that he struggled to open letters and needed reminders about appointments. They agreed to re-book an appointment and to set up telephone call reminders before his outpatient appointment.
On 6 June 2025, a letter was sent to the Service User inviting him to an outpatient psychiatrist appointment on 29 July 2025. A member of CMHT staff sent him a voice message on 10 June 2025 to advise him of this and to let him know that he would receive automatic text message reminders to his mobile phone. These reminders needed to be requested on an individual basis by CMHT staff, unlike the SPA team where this was automatic. The Service User was allocated a key worker on 21 July 2025 who contacted the Service User by telephone and confirmed his next appointment on 29 July 2025 with him. The Service User said that ‘everything is the same with him; he has a lot going on in his head and would appreciate a text’ reminder. The text reminder was set up and his key worker also telephoned the Service User to prompt him the day before his appointment.
The Service User attended his outpatient appointment on 29 July 2025 with the psychiatrist and his key worker. The psychiatrist gave the Service User information about his mental health condition so he could better understand what was happening and how to manage it and reassured him. They documented that the Service User was using alcohol and occasionally amphetamines, and therefore ‘strongly advised’ him to self-refer to a local drug and alcohol support service. His antidepressant and antipsychotic medications were changed, and the psychiatrist arranged the following:
- an electronic prescription for a 20-day supply of the new medication, sent to his nominated pharmacy
- an appointment for tests to monitor his physical health
- for his GP to stop a medication for anxiety as it could cause difficulty sleeping
- to have a home occupational therapy assessment (to assess what support might be needed to assist with everyday activities at home)
- a referral to the community social inclusion team to support the Service User with his independence.
On 30 July 2025 the Service User collected his new medication. His key worker also spoke with him by telephone and advised him to return his discontinued medication to the pharmacy. The key worker arranged to meet the Service User for an in-person appointment on 13 August 2025.
Between 6 August and 8 August 2025, the social inclusion team tried to telephone the Service User three times. These calls were not answered, and the Service User was discharged from that service.
On 9 August 2025 the Service User attempted to end his life. He was taken to hospital with serious injuries and treated for several weeks before being discharged home.
Investigation approach
Investigation team
| Role | Initials | Job title | Dept/directorate and organisation |
|---|---|---|---|
| Investigation commissioner/convenor: | This investigation is one of three PSII exemplars about mental health care | HSSIB | |
| Investigation lead: | The report is led by, and a publication of, HSSIB rather than any individual | HSSIB |
Summary of investigation process
The Service User’s sister telephoned the single point of access (SPA) service on 10 August 2025 and informed them that she had been contacted by the hospital the previous night to tell her about the Service User’s injuries. It was documented in the Service User’s healthcare records that his sister asked whether there had been any worsening in his mental health, as the mental health team usually telephoned her if the Service User was ‘unwell or not engaging’. The SPA mental health practitioner confirmed that ‘the Service User was engaging’. The Service User’s key worker telephoned the Service User’s sister the next day and reported the incident on the mental health trust’s local risk management system on 13 August 2025. The report was reviewed by the Trust’s patient safety team on 15 August 2025 when it was allocated for an After Action Review, a framework for debriefing after an incident (Health Services Safety Investigations Body, 2025a), on 28 August 2025.
In line with expected practice for NHS organisations, the incident was recorded on the Trust’s local incident database and identified as requiring a safety learning response. HSSIB had reached out to NHS mental health trusts and communities of practice to alert them of their intention to model PSIIs using the PSIRF framework on common topics that they might investigate. HSSIB and senior staff from the mental health trust that provided the Service User’s mental health care met to better understand if they could support this work. After discussion, it was agreed that the Service User’s experience would be the focus of one of three HSSIB investigations about mental health. The hospital stood down the planned After Action Review and worked with the HSSIB team during the investigation.
The draft report was shared for comments with the staff involved either directly or indirectly in the Service User’s care. These staff will also receive a final copy of the report once it has been approved by HSSIB. Progress on safety actions to address the areas of improvement included will be agreed and monitored by the relevant safety leads in the mental health trust.
Terms of reference
The terms of reference for this investigation were informed by information shared by the Trust. Key staff involved in the Service User’s care, either directly or indirectly, also helped to shape the areas of focus. The investigation intended to engage with the Service User for his input into the terms of reference; however, he did not wish to engage during the investigation.
This investigation will:
- explore the information provided by the GP in the Service User’s referral to secondary mental health services
- explore factors that influenced the care that the Service User received following receipt of their referral until they attempted suicide
- explore the support available to the Service User, his family and NHS staff providing care
- identify opportunities for improvement in the care pathway being investigated.
More details about the terms of reference, and how the investigation addressed these, can be found in appendix 1.
Information gathering
The investigation gathered information from multiple sources and sought different perspectives on events. The investigation considered how factors such as the environment, equipment, tasks, policies and organisational culture influenced the decisions and actions of staff. Information sources included:
- staff directly or indirectly involved in the Service User’s care
- the Service User’s GP and mental healthcare records
- national and local guidelines about care planning, assessment and management of clinical risk in mental health services, SPA service, community mental health team, promoting engagement, suicide, psychosis, and drug and alcohol use
- articles and research about community mental health services, suicide, self-harm, psychosis, and drug and alcohol use
- a suicide subject matter advisor (to mirror the local expertise available to mental health trusts).
Drawing on the ‘patient safety learning response toolkit’, the investigation used a number of different methods to help organise, understand and analyse the information gathered. Methods included:
- developing a timeline to help make sense and create a narrative understanding of events
- creating a stakeholder map – a map of all the relevant organisations, at different levels of the healthcare system, from government to hospital, to illustrate how these related to the activities of staff (see appendix 2)
- using a framework (called the Systems Engineering Initiative for Patient Safety (SEIPS)) to inform information gathering and help examine the data gathered. The framework prompts investigators to consider how work factors such as the environment, equipment, organisational policies and procedures interact to influence the actions and decisions of staff (see appendix 3)
- developing themes from analysis of the information gathered to help understand and explain why things happened in the way they did
- applying NHS England’s ‘Safety action development guide’ to inform thinking about the development of areas of improvement
- using an evidence log to document the information sources used to inform the investigation.
The investigation considered how far back to gather information about the Service User’s healthcare and decided to start from the time that he visited his GP to request a change in his antipsychotic medication. This point in time was agreed in order to complete the investigation in a timely way and in line with national expectations. The investigation also considered whether to contact the community pharmacy that dispensed the Service User’s medication but did not as this was beyond the terms of reference agreed for this investigation.
The investigation attempted to engage the Service User in the investigation process to capture his experience. This was limited at the Service User’s request and so the investigation does not include his reflections, or insights from those that supported him. During the investigation, considerations around service user engagement included carrying out welfare checks via the Service User’s key worker, understanding the Service User’s current mental health and considerations about how might be best to communicate with the Service User. Efforts to engage the Service User were revisited at the end of the investigation when the draft report was ready to determine whether he wished to see a copy. This was done via his key worker who confirmed the Service User did not wish to see the draft report or be named in the report.
Findings
This section sets out the findings from the investigation’s analysis of the information gathered. The investigation acknowledges that this may be incomplete as it was not possible to capture the Service User’s perspective, or that of his family or partner. For example, it was not possible to fulfil the term of reference about exploring the support provided to the service user or family (see appendix 1 – ToR 4).
The safety incident
The Service User’s attempt to end his life was not expected by the mental health staff supporting him. He was under the influence of alcohol at the time, and it is thought to have been an impulsive act. During their interactions with the Service User, staff from both the GP practice and community mental health service (CMHS) asked him about self-harm or suicidal thoughts. It was documented that the Service User did not report any such thoughts or actions. Factors that meant the Service User was more at risk of self-harm and suicide were documented, alongside protective factors that supported his mental health as part of his community mental health team (CMHT) assessment and safety plan.
The GP and CMHS staff also confirmed with the Service User that he knew how to seek help if his mental health declined. Best practice guidance published in 2025 noted that ‘Suicide prediction tools, scales, and stratification (for example, into low, medium, or high risk) are flawed because suicidal impulses are highly changeable and can shift in minutes’ (NHS England, 2025a). Instead, a relational and therapeutic engagement approach to safety assessment, planning and care is advocated and was mirrored by local Trust guidance. Not all suicide attempts can be prevented, but there remain opportunities for learning from the care provided to the Service User.
The findings are presented under the following headings:
- Information sharing and accessibility
- Personalised approach to care
- CMHT service demands versus resources
- Focusing on the community model of care.
Information sharing and accessibility
When the Service User first visited the GP to ask for a change to his medication, the GP identified that there were fewer prescription requests than expected if the Service User was taking the prescribed dose of his antipsychotic medication. It was documented that the Service User was not aware of the mismatch between what he had been taking and what was prescribed. The GP agreed with the Service User to increase his antipsychotic to the intended dose and review whether this controlled his symptoms after several weeks. This was not effective in controlling the Service User’s symptoms therefore he was referred to the CMHS.
The reason for referring the Service User to the CMHS was to seek specialist mental health input about his antipsychotic medication. The referral did not include any further information about the Service User’s previous mental health history, what prescribed medication he had previously tried and any side effects, or his concurrent alcohol and drug use. When asked, CMHS staff said their expectation was that the GP would provide the background detail as part of the referral. The investigation spoke with the Service User’s GP practice to understand further what information they chose to share about the Service User. The investigation was told it was unlikely that the GP who cared for the Service User would have any specific memory of their interaction. The investigation asked the single point of access (SPA) service staff if there was any local guidance available to support GPs referring service users to them. The investigation was not made aware of any local guidance.
The Service User had registered with his GP practice in 2020 and his GP was responsible for prescribing the Service User’s mental health medication. During this time the Service User had an inpatient mental health admission outside the local area, during which his current antipsychotic medication was started. His GP had taken over responsibility for the Service User’s mental health medication, including the antipsychotic. The records from the Service User’s inpatient stay were not accessible electronically to either the GP or CMHS.
The electronic healthcare record systems that the GP and CMHS use are not interoperable, meaning that information cannot be shared between the systems. Limited healthcare records are available via the NHS Summary Care Record (a digital extract of key information from a person’s GP record). Due to the limited information shared when the Service User was referred and the limited information available via the Summary Care Record, the CMHS was largely dependent on what the Service User told them to help them consider his needs. The lack of interoperability to enable records to be shared across and between health and social care providers to those authorised to access them is a national issue (Health Services Safety Investigations Body, 2025b).
The subject matter advisor highlighted the importance of having a deep understanding of who a person is and the experiences that have shaped their life alongside their medical history. Mental health support encompasses a service user’s physical health needs, mental health and social challenges in order to provide holistic care. Therefore background detail is key, yet there was no process for sharing the Service User’s needs to support his engagement with the CMHS following this referral. The investigation was unable to explore what processes the GP practice had in place to support this. The investigation noted that reliance fell on the unwell service user, who will have been asked to share the same insight on multiple occasions and may not be best placed to remember and/or share this information.
Area for improvement 1
Making information about service users easily available and accessible across providers to support effective initial engagement and decision making.
The investigation considered how information about the Service User was gathered following a referral by a GP to the SPA service. An SPA manager said that staff often contacted the referrer to gain additional information about the referral as part of their process. This information was then documented in the service user’s CMHS healthcare record, meaning it was available to authorised CMHS staff. The SPA team assessed the Service User’s eligibility for the different CMHS services available, and if appropriate onwards referred him or signposted him to other services. Changes to the Service User’s mental health symptoms, his compliance with prescribed medication, his drug and alcohol use, and the level of support available from friends/family at home were clearly documented in his healthcare records. This provided the CMHT staff with information about his progress while awaiting his medication review. During this time it was documented in the Service User’s healthcare record that he either stopped his antipsychotic medication ‘due to side-effects’ or took it ‘sporadically’. He had increased his alcohol consumption to ‘manage his symptoms’, ‘denied dependency’ and declined being referred to a community drug and alcohol service for support. The Service User stated his intention to reduce his alcohol use once his medication was changed and he therefore felt well enough to do so.
The investigation found that the Service User’s communication needs were not fully taken into account until he had missed appointments and months had passed. Reasonable adjustments to support his needs were then put in place (see ‘Personalised approach to care’ section). When asked what supported them to gain an understanding of a service user, the Service User’s key worker said there was “not an awful lot really”. They described reviewing the Service User’s healthcare records for relevant information including his diagnosis, outpatient appointments, and previous medical plans – whether or not these were followed. The key worker described that knowing about a service user’s drug and alcohol use was a “massive factor”. It took time to read a service user’s records, and this was part of the key worker’s role once the service user had been allocated a key worker.
People supporting a service user can, with the service user’s permission, provide useful insight into how the service user is coping. It was documented in the Service Users records that he had support from his son, partner and family but they were not involved in his triage or assessment. Local CMHS guidance promotes including those supporting a service user, when that is what the service user wants. This mirrors national ‘Staying safe from suicide’ guidance to ‘encourage the involvement of trusted others, where possible and as appropriate’ (NHS England, 2025a). The investigation was not able to seek the Service User’s view on whether or not he would have liked his son’s, family’s and partner’s input. The Service User’s key worker reflected that there was a ‘mismatch’ between the level of distress that the Service User was experiencing and how he seemed. It was not known whether involving those who supported the Service User would have allowed his ‘masking’ to be identified. Masking is when a person hides their true emotions, thoughts, or natural reactions so that other people do not notice them.
Personalised approach to care
The psychiatrist described a “working diagnosis of mental and behavioural disorder due to alcohol and amphetamine use”. The Service User was also described by the psychiatrist as being at the “pre-contemplative stage” of self change for substance misuse (Raihan and Cogburn, 2023) – that is, he retained capacity but was not yet considering a change in behaviour or was unaware of his need to change. The psychiatrist also explained that substance use causes changes in a person’s brain which affects their “ability to reason” and reduces their ability “to make informed choices”. The psychiatrist said that it is “very, very, very difficult to make a choice to stop using substances when you are still using”.
The investigation found the receipt of the GP referral and follow-on actions appeared to be streamlined to support the CMHS’s flow and process with service users who engaged. However, as the Service User missed three CMHT assessment and two psychiatrist outpatient appointments, this meant that he re-entered the pathway several times. During this time the Service User spoke with many different staff, from both the SPA service and CMHT, who had limited information upon which to tailor their engagement with him (see previous section). The investigation was unable to establish whether the Service User understood the different stages of the referral process.
From his healthcare records and discussions with staff that were not documented until he was transferred to the CMHT, the investigation found many factors that may have affected the Service User’s ability to engage with in-person appointments. These included his:
- tendency to sleep during the day when appointments may be scheduled
- need for support with written correspondence
- poor memory
- anxiety when in contact with other people
- need to walk or get a lift to attend appointments (there is no public transport from his home to the outpatient venue).
Staff told the investigation of the importance of service users having consistent staff to help build rapport, especially when engagement might be challenging. Due to CMHT capacity issues (see next section), the Service User was not allocated a key worker until July 2025. After this there was clear evidence of greater personalisation of the Service User’s care and planning by his key worker and psychiatrist. The Service User’s key worker found that the Service User did not read written correspondence sent to his home address and he also had dyslexia and had been diagnosed with attention deficit hyperactivity disorder. Examples of reasonable adjustments made were: planning telephone discussions for the morning when the Service User was still likely to be awake; calling him to remind him of any appointments; including how best to contact the Service User, and methods to avoid on the referral to the social inclusion team; the Service User’s phone was not set up to allow a voice message to be left, so staff tried calling back at a different time of the day or on another day.
CMHT staff explained that a blanket approach to supporting engagement may not be effective for all service users. For example, text reminders may help some people to remember appointments but could cause anxiety for others. This contrasted with the SPA team’s approach, where automatic text reminders for appointments were integral to their processes and did not account for individual service user preferences.
The Service User’s key worker told the investigation that service users who “don’t engage regularly” would be a higher priority, as it is a “red flag” for them being at risk. The subject matter advisor commented that the most “vulnerable” may be those who are “quietest”, but in reality staff “only” have capacity to prioritise those in crisis or who are very demanding.
Local CMHS guidance highlighted that the Service User was at risk of disengaging with services as he had both mental ill-health and concurrent drug and alcohol use. This reflects national guidance on maintaining contact between service users with both mental ill health and who also uses substances, were the need for a ‘proactive, flexible’ approach is highlighted (National Institute of Health and Care Excellence, 2016). Additional guidance issued to Integrated Care Boards highlighted that some people who experience psychosis may ‘struggle to access’ care and treatment. This guidance emphasised the importance of understanding when non-engagement may be due to mental ill-health, needing intensive support such as ‘assertive outreach’ (NHS England, 2025b). The CHMS local policy acknowledges that while service users have a choice about whether or not to access services, ‘it is imperative that all staff do not see disengagement automatically as a service user choice’. In addition, the CHMS local policy says: ‘Before any service user who uses substances/alcohol or both, is discharged from any service, there must be a clearly documented record of the discussion, and a clear onward plan identified, including details of any re-referral routes.’ Staff tried to understand the Service User’s reason for not attending but were not always successful in reaching him or his partner. His case was discussed with a manager on each occasion before he was sent an ‘opt-out’ which provided him with a way to ask for his support to be continued. This prompted the Service User to contact the CMHS and his appointments were rescheduled.
The investigation saw the dilemma the CMHS faced with limited resources (see next section) where there was a need to balance between gathering adequate information about a service user for triage and assessment by services they may be referred to and knowing where reasonable adjustments were needed to enable the service user to engage.
Area for improvement 2
Early exploration of adjustments that individual service users might need to engage in the triage and referral processes.
The change to his medication meant it was a potentially vulnerable time for the Service User's mental health. People with a ‘co-occurring disorder’, such as the Service User, are less likely to take their medication as prescribed. In the Service User’s case this was because he could not tolerate the side effects of the antipsychotic medication. The psychiatrist made a plan to change the Service User’s antidepressant to one that was less toxic if taken in overdose. The Service User was to start a new antipsychotic at a low dose and be reviewed in 2 weeks’ time. This was in line with local and national guidance (National Institute for Health and Care Excellence, 2014; 2022). This plan was individualised to accommodate the Service User’s continued alcohol use, while best managing his mental health symptoms with minimal medication side effects and monitoring any impacts on his physical health. The Service User was asked to return his other medication to the pharmacy for safe disposal, to mitigate the risk of self-harm.
The investigation noted several queries from CMHS mental health practitioners (MHPs) about whether medication could be prescribed for the Service User while he continued to drink alcohol and if that affected whether he was eligible for CMHT services. In addition, it was documented in his CMHT healthcare records that the Service User was advised, by non-medical CMHT staff, that he ‘had to be sober’ before the psychiatrist could prescribe him any medication. The psychiatrist explained that there were international evidence-based prescribing guidelines for how to do this. They also noted it was important that service users were supported to reduce alcohol use safely. If service users believed they might have to be sober to be eligible for prescribed medication this might act as a trigger to reduce their engagement with CMHS. National guidance recommends that ‘Healthcare professionals working within secondary care mental health services should ensure they are competent in the recognition, treatment and care of adults and young people with psychosis and coexisting substance misuse (National Institute for Health and Care Excellence, 2011).
Drug and alcohol services were available via a local partner organisation in line with national guidance (NHS England, 2019). The psychiatrist reflected that this created an additional barrier to service users taking up this support, and that if this had been available within the Trust, the Service User could have had a joint appointment and a collaborative plan could have been agreed. A CMHS staff member explained that when service users are supported by both the CMHS and a drug and alcohol service, CMHS staff do not have access to the service user’s drug and alcohol electronic health records, and vice versa, which sometimes posed a risk (see section on information sharing and accessibility). The key worker’s role includes co-ordinating care with other teams and partner organisations involved with the service user’s care. Several staff commented on the lack of widespread drug and alcohol support services as a national issue (Health Services Safety Investigations Body, 2025c), with little focus on early prevention.
Area for improvement 3
Staff knowledge and insight into how community mental health services can support service users who may require prescription medication and who use drugs and/or alcohol.
CMHT demand versus capacity
The investigation heard that the CMHS was under immense pressure with a mismatch between the resources available and demand. This meant that care had to be prioritised to those most in need and was having an impact on staff and service users. This reflected national issues. ‘The state of health care and adult social care in England 2024/25’ report (Care Quality Commission, 2025), showed a 15% increase in new referrals to secondary mental health services compared with 2022/23, lengthy waits, and that people’s needs were becoming increasingly complex.
The investigation was told that an increase in demand for mental health care at the same time as government funding cuts, shortages of experienced qualified mental health staff and concerns about whether staff trained overseas would continue to be supported, contributed to the mismatch between available resources and demand. The investigation explored how these factors affected the CMHT that the Service User was referred to.
The mental health trust community services divisional leadership team shared that the CMHT had “greater pressures” including from service users with “more acuity [more severe mental health conditions] … more complexity” and “physical health issues, generational issues, deprivation issues”. They also said drug and alcohol use had become more common. The CMHT service manager explained that services were not commissioned by volume (payment was a flat fee, rather than relating to total number of service users service were provided to) and both they and the divisional nurse felt they were “overdelivering” based on unmet need. The investigation was told that there were ongoing discussions between the mental health trust and the commissioners. For example, several staff explained they were experiencing “significant push back” from some GPs about taking back the care of service users who were stabilised on long-term medication, via shared care arrangements, due to the “oversight costs”. This meant that the CMHT needed to support these service users while this was being resolved.
The Trust had undergone a transformation several years ago to align with the Community Mental Health Framework for Adults and Older Adults (NHS England, 2019), and transformation activities were ongoing to further refine and develop the CMHS. During interviews staff sometimes referred to previous teams and arrangements and were not always clear on the role and responsibilities of current teams. These staff suggested that this contributed to service users being inappropriately referred, where the receiving team were unclear why the service user had been referred or were unable to offer any interventions. This created additional workload because of the need to follow up to find out more about the referral and/or meant disappointing the service user if they did not meet the service’s referral criteria. The investigation was told that collaborative work was ongoing to review referrals from the SPA service to the CMHT. An SPA service staff member said that some referrals “do not fit in a box” but needed to go somewhere and explained that they needed the local teams’ referral criteria to be more flexible.
Staff described concerns that the CMHT was “carrying more risk” than it used to. For example, one staff member said that: “… everyone is stretched to capacity … [there is] just not enough manpower to cover the risk of the patients that we have with what we’ve got. Never mind when one or two of those [staff] are off sick.” Staff said that other local services were “passing issues back” to the CMHT to resolve. This ranged from other local CMHS teams which the investigation were told “used to work collaboratively”, to the ambulance service or local accident and emergency department not accepting a service user unless their key worker waited with them. The investigation also heard that it was more challenging to get service users accepted by other teams. A staff member described this as feeling like “teams were working to reject referrals”, while another described it as “working in silos”.
Staff described having to prioritise which tasks they did; for example, one staff member said that “when pushed the first thing that drops is documentation”. This potentially affected the availability of information for other CMHS staff members. The investigation was told of a situation where the safety of a staff member was compromised because the risk of harm to others by a service user was not highlighted in the service user’s records.
Because of capacity issues, the CMHT has a procedure to determine which service users are high priority and these are allocated a key worker. Other service users may be placed on a waiting list until there is capacity for them to be allocated a key worker. Arrangements are in place to maintain periodic contact with these service users, to ensure they know how to seek assistance and ask for more support if needed. This task is part of the ‘duty worker’ role.
The investigation spoke with the MHP covering the duty worker role who explained that, with over 100 unallocated service users on the waiting list, it was a very busy role which posed a risk of “things getting missed”. They also said that when the CMHT was fully staffed the number of unallocated service users fell, but with staff sickness numbers had risen. An MHP told the investigation that staff “dread [covering] it” due to the heavy workload that can then “eat into their other work”. A staff member explained that service users got “very frustrated” because they wanted to be allocated a key worker, which could take months, and they spoke with a different MHP each time. A part-time substantive duty worker had recently been appointed to provide consistency.
The CMHT service manager described variation in the different CMHTs' they were responsible for, with those based in the city being “exceptionally busy” and having issues “maintaining staff due to frequency of burnout”, high “quite demanding caseloads” and a “considerable amount of complex cases”. Each key worker had up to 30 service users on their caseload. The investigation learned that there was a risk on the divisional risk register relating to an “increase in [staff] vacancies and long term sickness resulting in care delays and poor patient experience due to the number of unallocated” service users. The CMHT and divisional management staff carried out weekly reviews of CMHT performance via a live dashboard, which allowed them to monitor the impact on teams and service users to manage this dual staff and patient safety hazard.
It was clear from speaking to staff that the above factors had an impact on the staff working in the CMHT. The investigation heard of several staff members having had long-term sickness absence, either in the months leading up to the investigation’s visit, or during the time of the visit. Staff described burnout being a common reason for sickness absence and feeling overwhelmed because of the consistently high caseloads they carried. They talked about the “general pressure” they felt, in part due to “not having enough time [to do the work they need to]”. Managing such pressures and supporting staff to maximise their wellbeing is important for the sustainability of services.
The investigation was told of a clinical supervision model that was in place across the CMHT which provided staff with an opportunity to talk about any challenges at work and discuss cases. When speaking to staff about supervision, many told the investigation that this was often cancelled because of lack of capacity and availability of those delivering the supervision. This meant staff members were often going for long periods of time without a formal supervision session. Restorative clinical supervision has a number of roles including: giving staff space to deal with the distress they encounter during their role, allowing staff to reflect on their inherently complex practice and strengthen their clinical judgement.
Despite the pressures on the team, staff within the CMHT felt there was a good team rapport. They described supporting each other well which helped to maintain morale in the team and some of them said this was the reason they stayed working in the team. Staff described particular challenges with a lack of consistent CMHT leadership because of staff sickness. The investigation noted the working environment appeared very calm. Staff were doing their best to support service users and wanted to be able to do more; however, this was not possible without adversely affecting their own wellbeing.
Following the site visit the investigation explored with management teams the support available to staff. Initiatives and processes exist such as clinical supervision and a wellbeing offer to staff which they can access via the intranet should they wish to. Management teams were keen to support staff and try and improve the situation described above. However there appeared to be a disconnect between the intention to improve staff wellbeing and the ability to achieve this on the frontline. The Trust’s most recent Care Quality Commission inspection report had similarly noted high vacancy rates and low but improving rates of supervision and annual appraisal.
The divisional team leader acknowledged the risk of work-based trauma because of the nature of the CMHT role and said this was “already on their radar” as a local and national “area of concern”. Staff may feel responsible or blamed when a service user comes to harm, yet “it is difficult to disentangle the potential for prevention, if any, by mental health services” (Averill et al, 2023). A number of different types of support were suggested to the investigation including: clinical or restorative supervision, professional nurse advocates, defusing and debriefing after incidents. The subject matter advisor told the investigation that there is forthcoming national guidance from the Royal College of Psychiatrists recommending team reflective practice.
Area for improvement 4
Organisational support for protected time, resources and assistance for staff to mitigate and respond to the distress and demands they experience in their role.
NHS England’s ‘Staying safe from suicide’ guidance recommends a three-step safety approach consisting of safety assessment, dynamic safety formulation, and safety management and planning (NHS England, 2025a). This approach allows the team to take a moment to stand back and reflect on what is known following a service users attempt to take their life, consider whether other expertise might be useful, and use this new insight to ‘create a shared understanding of current problems with safety’ and develop a ‘collaborative safety plan to manage future changes in safety and review it regularly’. Here safety refers to both service user, family and staff safety. The mental health trust used a safety formulation model as part of care planning and local policy required that this was updated as needed. The ‘Staying safe from suicide’ guidance appeared to the investigation to be an enhancement on what was currently in place.
Focusing on the community model of care
The investigation reflected on how the Trust was continuously trying to transform its services to meet the the national CMHS recommendations (NHS England, 2019). It was unable to gain the Service User’s thoughts or experiences so the investigation’s considerations are limited to what staff shared that may be relevant to the Service User’s experience.
Staff explained that caring for mentally unwell people in the community has challenges. Providing mental health care in a community setting is highly complex, where the CMHS has ‘wider responsibility to care for the ‘whole person’’ (Averill et al, 2023), but does not have control of many of the factors that may affect the service user. Lots of interactions are remote, with no available visual cues about the service user and their environment. Several staff said there was a perception that service users who are being supported in the community are “more stable” than those being cared for as inpatients. However, community staff were “spread thinly” compared to recommended staffing levels for mental health inpatient care.
CMHS resources were affected by fluctuations in staffing and funding instability. The investigation heard that the current cost saving and historical reliance on the Mental Health Investment Standard (NHS England, 2025c) (dedicated funding to support increased spending on mental health services) for the CMHTs' was a concern. The Trust was in discussion with the integrated care board and NHS regional teams about these plans and was keen to be more involved in commissioning conversations. However, the investigation was told that ‘out of area placements’ (inpatients being placed in care settings far from their own geographical area) were dominating discussions with the integrated care board and continued reliance on inpatient mental health care meant that funding spent in this way could not be redirected towards CMHTs'. This mirrors national concerns about mental health funding arrangements to ensure ‘parity of esteem’ with physical healthcare (Care Quality Commission, 2025; Health and Social Care Committee, 2025). Similarly, national staff recruitment and retention issues have created gaps in staff experience and competency, further adding to pressure to services with staff ‘feeling burnt out and overworked, and that they are constantly fighting fires, with little long-term impact’ (Care Quality Commission, 2025).
Summary of findings and areas for improvement
The investigation found that:
- The Service User’s attempt to end his life was not expected by the mental health staff supporting him.
- The change to his medication meant it was a potentially vulnerable time for the Service User's mental health. This was despite him having a safety plan for how to seek help if he felt overwhelmed and planned monitoring check-ins in line with local procedure.
- The Service User’s case was complex and challenging; his mental ill-health, drug and alcohol use are likely to have impacted on his ability to reason and make informed decisions. Therefore, sharing of information across and between healthcare services was important to facilitate personalised care planning.
- Limited sharing of, and lack of ready access to, information about the Service User and his past mental health history impacted on the CMHS’s ability to provide effective and timely care.
- The Service User needed a tailored approach with reasonable adjustments to maximise his engagement with mental health services; there was a delay in his needs being identified and acted on.
- There was limited understanding and awareness by some staff of whether mental health medication can be offered to service users with mental health issues and concurrent alcohol use.
- Staff worked in a service that was overstretched and qualified healthcare professionals had to make decisions about managing service user needs, service demand, and risk and safety, within limited resources. The demand for CMHT services exceeded the available capacity, impacting both service users and staff.
- Staff did not have the dedicated time and space to process and deal with distress they encountered as part of their daily work caused by incidents of patient harm.
- There are challenges to delivering the national ambition to provide a community focused model of care, many of which the mental health trust has limited or no control over.
Summary of areas for improvement
The investigation identified four areas of improvement which the mental health trust could develop safety actions to address.
Area of improvement 1
Making information about service users easily available and accessible across providers to support effective initial engagement and decision making.
Area of improvement 2
Early exploration of adjustments that individual service users might need to engage in the triage and referral processes.
Area of improvement 3
Staff knowledge and insight into how community mental health services can support service users who may require prescription medication and who use drugs and/or alcohol.
Area of improvement 4
Organisational support for protected time, resources and assistance for staff to mitigate and respond to the distress and demands they experience in their role.
Appendices
Appendix 1: Terms of reference (ToR)
| Incident/incident reference | (I-034394 HSSIB) |
|---|---|
| Date agreed/version no. | 5 November 2025 |
| Date investigation is to be completed by | 2 April 2026 |
| Learning response lead | HSSIB |
| Staff engaged in the development of ToR (names/roles) |
The investigation approach was discussed with the staff interviewed, but they were not directly involved in the with development of the ToR. HSSIB staff. |
| Patient/family/carers engaged in the development of ToR (names/relationship) | Offered to share with Service User but declined. |
| Name | |
| Relationship |
The investigation will:
| ToR 1 | Explore the referral made for the Service User to mental health services in October 2024 |
|---|---|
| Key questions |
List of questions to be asked to support the aim of the ToR: 1. What was known about the Service User’s past mental health history, his preferences and how best to engage with him? Specifically, had he previously self-harmed, attempted suicide or had suicidal thoughts? 2. Why was the Service User referred to mental health services? 3. What information was communicated in the referral to mental health services? 4. What supports and challenges the current referral process? |
| Healthcare settings |
Key areas considered relevant to observe/interact with during the investigation: • GP practice where the Service User was registered • The Service User’s home. |
| Healthcare processes |
Known processes that appear significant to consider within the investigation: • GP assessment that the Service User needed specialist mental health input to review his prescribed medication • Process for a GP referring a person to mental health services • Access to healthcare records from providers where the Service User had previously received mental health care. |
| ToR 2 | Explore the care provided to the Service User following receipt of the referral until he was allocated a key worker |
|---|---|
| Key questions |
List of questions to be asked to support the aim of the ToR: 1. What information was available to the staff deciding on the Service User’s care pathway? 2. What processes existed to support staff decision making about the Service User’s treatment? 3. How was information about the Service User’s care needs and treatment shared within and across those teams involved with his care? 4. How was the Service User communicated with about his care during this time? 5. How did staff deal with the complexity of supporting the Service User, who might struggle to engage or not wish to accept treatment recommendations? 6. What safety hazards are there with the current process and how are these mitigated? |
| Healthcare settings |
Key areas considered relevant to observe/interact with during the investigation: • GP practice • Mental health trust (SPA service and CMHT) • The Service User’s home. |
| Healthcare processes |
Known processes that appear significant to consider within the investigation: • SPA service to understand referral receipt, triage and assessment regarding the Service User’s treatment pathway • How the CMHT duty worker role is carried out (including checking in on people whose cases have not yet been allocated) • How eligibility for CMHT care is decided • CMHT – medication review and key worker roles in relation to the Service User’s care provision. |
| ToR 3 | Explore the care provided to the Service User from when he was allocated a key worker until his attempt to take his life |
|---|---|
| Key questions |
List of questions to be asked to support the aim of the ToR: 1. What information was available to the staff deciding on the Service User’s care pathway? 2. How was the decision about the Service User’s treatment made? 3. How was information about the Service User’s treatment shared within and across those teams involved with his care? 4. How did staff deal with the complexity of supporting service users who might struggle to engage or not wish to accept treatment recommendations? 5. How was the Service User communicated with about his care during this time? 6. What safety hazards are there with the current process and how are these mitigated? |
| Healthcare settings |
Key areas considered relevant to observe/interact with during the investigation: • GP practice • Mental health trust (CMHT (outpatient psychiatrist appointment and key worker) and social inclusion service) • The Service User’s home. |
| Healthcare processes |
Known processes that appear significant to consider within the investigation: • Escalation processes if the Service User was not coping with his mental health (by those supporting the Service User as well as by healthcare staff) • Social inclusion service triage, engagement and discharge processes • Staff support for learning/reflection from safety events. |
| ToR 4 | Explore the support available to the Service User, his family, and NHS staff providing his care? |
|---|---|
| Key questions |
List of questions to be asked to support the aim of the ToR: 1. Were staff able to tailor their care approach to the Service User’s needs? 2. What safety hazards are there with the current process and how are these mitigated? 3. What infrastructure is available to support the Service User, his family and staff who may have been impacted by the complexity of care/the attempted suicide? |
| Healthcare settings |
Key areas considered relevant to observe/interact with during the investigation: • GP practice • Mental health trust (CMHT and patient safety team) • The Service User’s home. |
| Healthcare processes |
Known processes that appear significant to consider within the investigation: • Documentation and visibility of information about the Service User’s needs and preferences • Access to healthcare records from previous mental health care providers • Staff support for learning/reflection/processing potentially traumatising events • Support for the Service User/his family during this time • Engaging with the Service User’s wider circle of support to build a picture of his needs, preferences and support during difficult times/when well. |
Appendix 2: Stakeholder Map
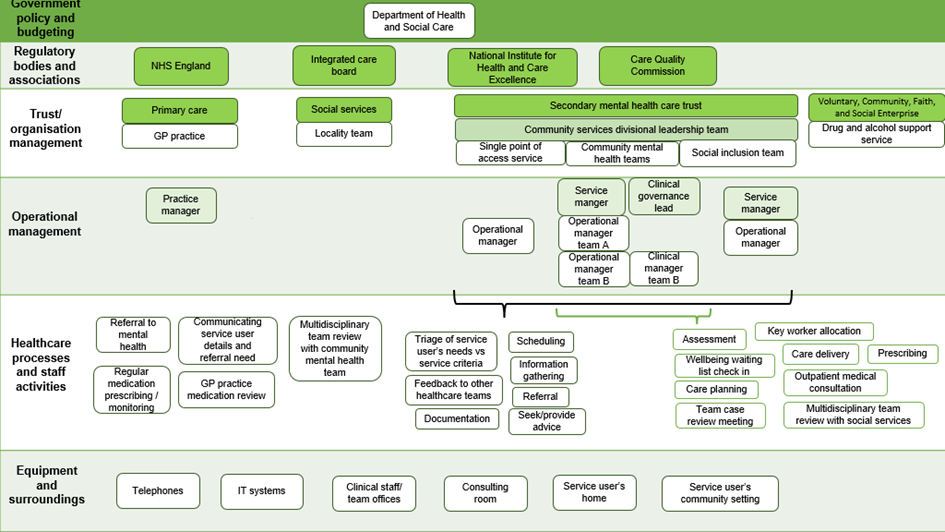
Appendix 3: Systems Engineering Initiative for Patient Safety (SEIPS) framework
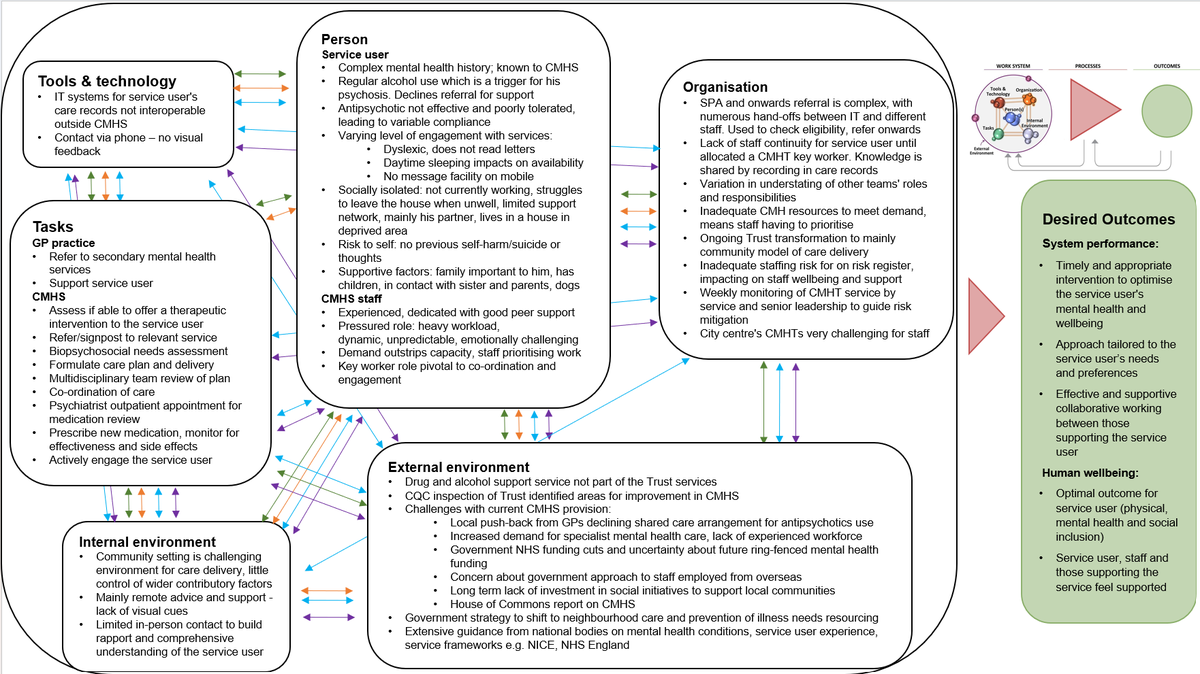
Abbreviations used in Appendix 3:
CQC – Care Quality Commission
CMHS – Community mental health service
SPA – Single point of access team
CMHT – Community mental health team
NICE – National Institute for Health and Care Excellence
CMHF – Community mental health framework
Appendix 3 key interactions
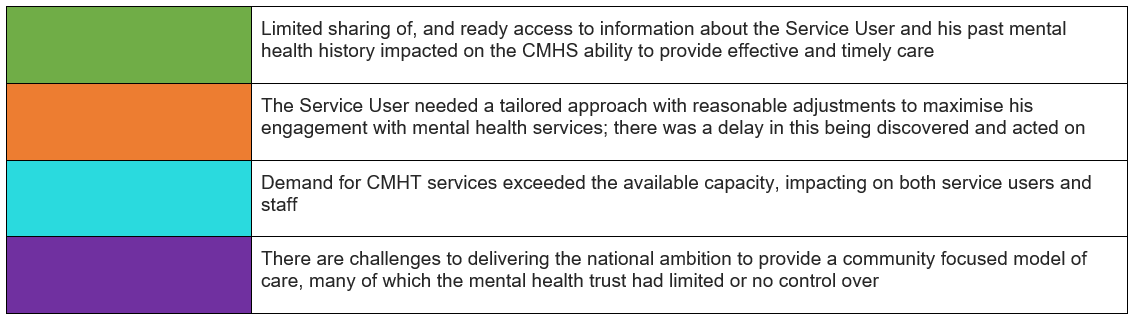
References
Alcohol Change UK (n.d.) Understanding the language around different patterns of drinking. Available at https://alcoholchange.org.uk/policy/policy-insights/understanding-the-different-patterns-of-drinking (Accessed 9 February 2026).
Alcohol Change UK (2025) Alcohol and mental health. Available at https://alcoholchange.org.uk/alcohol-facts/fact-sheets/alcohol-and-mental-health (Accessed 9 February 2026).
Anderson, L.A. (2025) Antipsychotic medications and alcohol interactions. Available at https://www.drugs.com/article/antipsychotic-medications-alcohol.html (Accessed 9 February 2026).
Taylor, D.M., Barnes, T.R.E., et al (2026a) Addictions and substance misuse, in The Maudsley Prescribing Guidelines in Psychiatry: John Wiley & Sons, Ltd, pp. 477–560. Available at https://onlinelibrary.wiley.com/doi/10.1002/9781119870203.mpg004.pub2 (Accessed 9 February 2026).
Taylor, D.M., Barnes, T.R.E., et al (2026b) Depression and anxiety disorders, in The Maudsley Prescribing Guidelines in Psychiatry: John Wiley & Sons, Ltd, pp. 335–476. Available at https://onlinelibrary.wiley.com/doi/10.1002/9781119870203.mpg003.pub2 (Accessed 9 February 2026).
Averill, P., Vincent, C., et al. (2023) Conceptual and practical challenges associated with understanding patient safety within community-based mental health services, Health Expectations, 26(1), pp. 51–63. doi: 10.1111/hex.13660
Care Quality Commission (2025) The state of health care and adult social care in England 2024/25: Mental Health. Available at https://www.cqc.org.uk/publications/major-report/state-care/2024-2025/access/mh (Accessed 9 February 2026).
Health and Social Care Committee (2025) Community mental health services: fourth report of session 2024-26 HC 566. Available at https://committees.parliament.uk/publications/50484/documents/274145/default/ (Accessed 9 February 2026).
Health Services Safety Investigations Body (2025a) After Action Review. Available at https://www.hssib.org.uk/education/resources/after-action-review/ (Accessed 9 February 2026).
Health Services Safety Investigations Body (2025b) Electronic patient record (EPR) systems – thematic review. Available at https://www.hssib.org.uk/patient-safety-investigations/electronic-patient-record-epr-systems-thematic-review/ (Accessed 10 February 2026).
Health Services Safety Investigations Body (2025c) Mental health inpatient settings: overarching report of investigations directed by the Secretary of State for Health and Social Care. Available at https://www.hssib.org.uk/patient-safety-investigations/mental-health-inpatient-settings/fifth-investigation-report/ (Accessed 10 February 2026).
Mayo Clinic (2022) Alcohol use disorder. Symptoms and causes. Available at https://www.mayoclinic.org/diseases-conditions/alcohol-use-disorder/symptoms-causes/syc-20369243 (Accessed 9 February 2026).
Mental Health Foundation (2022) The truth about self-harm for young people and their friends and families. Available at https://www.mentalhealth.org.uk/sites/default/files/2022-07/MHF-The-truth-about-self-harm-guide.pdf (Accessed 9 February 2026).
National Institute for Health and Care Excellence (2011) Coexisting severe mental illness (psychosis) and substance misuse: assessment and management in healthcare settings. Clinical guideline 120. Available at https://www.nice.org.uk/guidance/cg120/resources/coexisting-severe-mental-illness-psychosis-and-substance-misuse-assessment-and-management-in-healthcare-settings-pdf-35109443184325 (Accessed 31 March 2026).
National Institute for Health and Care Excellence (2014) Psychosis and schizophrenia in adults: prevention and management. Clinical guideline CG178. Available at https://www.nice.org.uk/guidance/cg178 (Accessed 9 February 2026).
National Institute for Health and Care Excellence (2016) Coexisting severe mental illness and substance misuse: community health and social care services. NICE guideline NG58. Available at https://www.nice.org.uk/guidance/ng58/chapter/Recommendations#maintaining-contact-between-services-and-people-with-coexisting-severe-mental-illness-and-substance (Accessed 10 February 2026).
National Institute for Health and Care Excellence (2022) Depression in adults: treatment and management. NICE guideline NG222. Available at https://www.nice.org.uk/guidance/ng222 (Accessed 9 February 2026).
NHS (2023a) Overview – Psychosis. Available at https://www.nhs.uk/mental-health/conditions/psychosis/overview/ (Accessed 9 February 2026).
NHS (2023b) Treatment – Psychosis. Available at https://www.nhs.uk/mental-health/conditions/psychosis/treatment/ (Accessed 9 February 2026).
NHS (2023c) Why people self-harm. Available at https://www.nhs.uk/mental-health/feelings-symptoms-behaviours/behaviours/self-harm/why-people-self-harm/ (Accessed 9 February 2026).
NHS (2025) Antidepressants. Available at https://www.nhs.uk/medicines/antidepressants/ (Accessed 9 February 2026).
NHS England (n.d.) Mental health practitioners. Available at https://www.england.nhs.uk/mental-health/working-in-mental-health/mental-health-practitioners/ (Accessed 9 February 2026).
NHS England (2019) The community mental health framework for adults and older adults. Available at https://www.england.nhs.uk/publication/the-community-mental-health-framework-for-adults-and-older-adults/ (Accessed 9 February 2026).
NHS England (2025a) Staying safe from suicide. Best practice guidance for safety assessment, formulation and management. Available at https://www.england.nhs.uk/publication/staying-safe-from-suicide/(Accessed 9 February 2026).
NHS England (2025b) Guidance to integrated care boards on intensive and assertive community mental health care. Available at https://www.england.nhs.uk/long-read/guidance-to-integrated-care-boards-on-intensive-and-assertive-community-mental-health-care/ (Accessed 31 March 2026).
NHS England (2025c) Mental Health Investment Standard (MHIS): categories of mental health expenditure. Available at https://www.england.nhs.uk/long-read/mental-health-expenditure-categories/ (Accessed 9 February 2026).
Raihan, N. and Cogburn, M. (2023) Stages of change theory, in Raihan, N. and Cogburn, M. (eds.) Treasure Island (FL): StatPearls Publishing. Available at https://www.ncbi.nlm.nih.gov/books/NBK556005/ (Accessed 9 February 2026).
Mental health trust guidance
Assessment and management of clinical risk in mental health services policy and procedure (2024).
Effective care planning in mental health and learning disability services policy (2024).
Promoting engagement and access to mental health services procedure (2024).
Single point of access (SPA) service policy and procedures (2025).
Community mental health team (CMHT) procedure (2025).
Unallocated cases (under CMHT) procedure (2025).
Procedure for the monitoring of psychotropic medication (2025).
Co-occurring disorder and addiction policy (2025).
Medicines management shared-care guideline – second-generation antipsychotics (2023).