A note of acknowledgement
We would like to thank the patients and people in prison who engaged with the investigation. Their experiences and thoughts about the healthcare and social care they have received are central to the investigation and to the improvement of these services for people in prisons. We would also like to thank the healthcare and prison staff who engaged with the investigation for their openness and willingness to support improvements in this area of care.
About this report
This report is intended for healthcare and justice organisations, policymakers and the public to help improve patient safety in relation to the delivery of health and social care in prisons.
Executive summary
Background
This investigation focuses on how the health needs of people in prison are assessed and the provision of safe living conditions for people in prison who use a wheelchair or have mobility issues.
This is the fourth and final HSSIB report in a series on the theme of healthcare provision in prisons. The first report explored emergency care response, the second explored continuity of care and the third looked at data sharing and IT.
These investigations were launched after discussions with 26 national organisations across the healthcare and justice systems, through which HSSIB gained knowledge of their concerns about healthcare in prisons.
Through a patient engagement group, HSSIB engaged with more than 120 people in prison to understand their experiences of receiving primary healthcare (such as seeing a GP) and secondary healthcare (such as going to a specialist clinic or going into hospital). The investigation also engaged with stakeholders from across the prison healthcare system to gather evidence about primary and secondary patient care from their perspectives.
This investigation explored how healthcare provision for a whole prison’s population is assessed and commissioned using health needs assessments. How outdated assessments may present a patient safety risk through mismatched staffing skill mix and services that don’t match the patient’s needs. These risks may result in physical injuries, psychological distress and dignity violations, each of which can impact on patient wellbeing. It looked at challenges related to this approach, cost implications of the current system and ongoing developments.
Disability access within prisons is complicated by the original design and purpose of prison buildings. Some of the prison estate dates back as far as 1800, making adaptations and provision for wheelchair users, for example, difficult. The investigation explored the prevalence of this issue, the impact on people in prison and potential areas for improvement.
Findings
The investigation explored two main themes: health needs assessments and access for physically disabled people within prisons. These themes were identified during the evidence gathering phase for the three previous HSSIB reports in this series.
The findings have been separated into these two themes and are listed below:
Health needs assessments (HNAs)
- The current process of developing an HNA for a prison population, which are generally conducted at most every 3 years, means that HNAs are frequently out of date by the time they inform commissioning decisions.
- There is often a delay in prison healthcare providers being made aware of likely changes to the prison population by HM Prison and Probation Service (HMPPS). This can impact on providers’ ability to ensure the required healthcare provision is in place to serve the new population.
- Outdated HNAs lead to mismatched healthcare provision, forcing providers to submit business cases for additional services or absorb the financial impact of changes to their services.
- The business case processes were slow and did not support the needs of a rapidly changing prison population, resulting in services that may pose patient safety risks due to mismatched healthcare services, incorrect staff skill mix requiring retraining, recruitment, and removal/addition of new services.
- HNAs were commissioned by NHS England regional commissioning teams and did not include social care requirements as this is commissioned by local authorities, which made planning and provision of social care difficult and often resulted in delays in care.
- In response to limitations in the current HNA process, some regions had introduced alternative approaches, including digital data dashboards and artificial‑intelligence‑enabled tools.
- Different approaches to assessing healthcare requirements for prison populations contributed to variation in how healthcare services were commissioned and delivered across the prison estate.
- Stakeholder engagement in assessing prison population health requirements was limited; local authorities and other relevant bodies were rarely consulted, contrary to guidance.
Physical disability access
- Wheelchair users experienced harm and dignity concerns, including injuries from unsafe chair-to-chair transfers and deteriorating mental health caused by being housed in inappropriate accommodation.
- The number of wheelchair users in prisons is increasing, and many prisons cannot easily accommodate wheelchair users or people with mobility issues.
- None of the prisons visited had enough wheelchair-accessible cells. In some regions there were none.
- Accessible cells are sometimes located only on vulnerable prisoner wings, potentially wrongly associating wheelchair users with that cohort of prisoners.
- The current system for gathering information on the physical accommodation needs of people in prison is ineffective; this can impact on the ability to place people in appropriate accommodation.
HSSIB makes the following safety recommendations
Safety recommendation R/2026/079:
HSSIB recommends that HM Prison and Probation Service, in collaboration with the Department of Health and Social Care, formalises arrangements for alerting healthcare commissioners and providers to changes in prison populations likely to impact on healthcare provision requirements. This is to ensure that healthcare commissioners and providers can plan for changes to healthcare services that are necessary to meet the changing needs of the prison population.
Safety recommendation R/2026/080:
HSSIB recommends that the Department of Health and Social Care works with local authorities to redesign how the health and social care needs of prisons’ populations are assessed. This is to ensure that appropriate services are commissioned to meet the needs of people in prison and prevent possible delays in care.
Safety recommendation R/2026/081:
HSSIB recommends that HM Prison and Probation Service reviews and amends its information gathering processes for accommodation requirements for wheelchair users and people with mobility issues, to identify and mitigate risks for people whose accommodation does not meet their needs. This is to enable and support the effective identification of appropriate prison accommodation for these groups.
1. Background and context
1.1 Introduction
1.1.1 This investigation focuses on the provision of health and social care and disability access for people in prison. In particular it explores:
- how the healthcare needs of people in prison are assessed, particularly those with social care needs
- what measures are in place for wheelchair users, including access to their cells and facilities within the prison.
1.1.2 The information in this section provides context for the analysis and findings in section 2.
1.2 Ministry of Justice
1.2.1 The Ministry of Justice (MoJ) is the government department responsible for the justice system.
1.2.2 The justice system includes:
- courts
- prisons
- probation services
- attendance centres (Ministry of Justice, n.d.a).
1.3 HM Prison and Probation Service
1.3.1 HM Prison and Probation Service (HMPPS) is an executive agency sponsored by the Ministry of Justice. It works with partner organisations to enable the sentences of the courts to be carried out, either in custody or the community.
1.3.2 Within England and Wales, HMPPS is responsible for:
- running prison and probation services
- rehabilitation services for ex-offenders leaving prison
- making sure support is available to stop people re-offending
- managing contracts for private sector prisons and services such as the Prisoner Escort and Custody Service and Electronic Monitoring Service.
1.3.3 Through HM Prison Service it manages public sector prisons and the contracts for private prisons in England and Wales.
1.3.4 Through the National Probation Service it oversees probation delivery in England and Wales including through community rehabilitation companies.
Prison categories
1.3.5 Prisons are categorised according to the risks associated with the prisoners they hold. There are four categories of prison for male prisoners:
- ‘Category A
These are high-security prisons. They house male prisoners who, if they were to escape, pose the most threat to the public, the police or national security. - Category B
These prisons are either reception or training prisons. Reception prisons house prisoners that are taken directly from court in the local area (sentenced or on remand), and training prisons hold long-term and high-security prisoners. - Category C
These prisons are training and resettlement prisons; most prisoners are located in a category C. They provide prisoners with the opportunity to develop their own skills so they can find work and resettle back into the community on release. - Category D – open prisons
These prisons have minimal security and allow eligible prisoners to spend most of their day away from the prison on licence to carry out work, education or for other resettlement purposes.’ (Ministry of Justice, n.d.b)
1.3.6 There are two categories of prison for female prisoners: open or closed. High-risk female prisoners are classed as ‘restricted status’ and are housed in closed prisons (Ministry of Justice, n.d.b).
Prison population and accommodation expansion
1.3.7 The prison population has been increasing steadily, with successive governments releasing plans to deal with a shortage of available prison accommodation. As the MoJ describes:
‘As of 2 December 2024, the population of the adult prison estate was 85,688, compromising (sic) 82,193 in the adult male estate and 3,495 in the women’s estate. The prison population has been under considerable pressure for some time, with the adult male estate running at over 99% capacity for much of the 18 months since February 2023.’ (Ministry of Justice, 2024a)
1.3.8 The 10-year prison capacity strategy produced by the MoJ (2024a) details how it will increase the size of the prison estate. This will be done through four key strategies:
- new prisons – around 6,500 places
- new houseblocks – around 6,400 places
- rapid deployment cells – around 1,800 places
- refurbishments – around 350 places brought back into use.
1.4 Prison healthcare
Equivalent care
1.4.1 The House of Commons Health and Social Care Committee report on prison health states that:
‘Prison health and care services should be delivering standards of care, and health outcomes, for prisoners that are at least equivalent to that of the general population.’ (House of Commons Health and Social Care Committee, 2018)
1.4.2 The Royal College of General Practitioner’s definition of equivalence reads:
‘‘Equivalence’ is the principle by which the statutory, strategic and ethical objectives are met by the health and justice organisations (with responsibility for commissioning and delivering services within a secure setting) with the aim of ensuring that people detained in secure environments are afforded provision of or access to appropriate services or treatment (based on assessed need and in line with current national or evidence-based guidelines) and that this is considered to be at least consistent in range and quality (availability, accessibility and acceptability) with that available to the wider community in order to achieve equitable health outcomes.’ (Royal College of General Practitioners, 2018)
Prison healthcare commissioning
1.4.3 In 2012 the Health and Social Care Act directed that healthcare services in prisons in England should be commissioned by NHS England. This responsibility was transferred to NHS England in 2013. NHS England commissions services through regional teams, with oversight from a central national team. Throughout this report the NHS England Health and Justice specialised commissioning regional teams are referred to as NHS England regional teams.
1.4.4 NHS England regional teams use the principle of equivalence when commissioning healthcare in prisons. This means that people who are detained by the justice system should receive an equivalent level of health service to the rest of the population.
1.4.5 NHS England, through its regional teams, is also responsible for quality assurance within the commissioned services, which aims to ensure service providers meet their contractual obligations and deliver services to the required standards.
1.4.6 During the investigation it was announced that NHS England was being abolished and elements were being merged into the Department of Health and Social Care (DHSC). It is intended that the national NHS England Health and Justice team will move into the DHSC, while the NHS England regional teams will become part of integrated care systems, as described by The King’s Fund (2025).
Prison healthcare departments
1.4.7 Each prison has a healthcare department that provides medical services to patients within the prison.
1.4.8 Healthcare departments provide different levels of cover depending on the commissioning requirements of the prison and its population. Most departments are nurse-led with GP-run clinics. Some departments provide 24/7 care, while others only provide daytime cover and some have no cover at weekends.
1.5 Health needs assessments
1.5.1 A health needs assessment (HNA) is a method for reviewing the health requirements of a prison population. The aim of HNAs is to help commissioners to provide health services by informing them of health priorities and identifying the resources required to improve health and reduce inequalities. HNAs are different from the individual health and social care needs assessments carried out in the community and within prisons that are specific to individual patients (discussed further at 2.1). They were introduced in 2014 to bring a level of consistency to how the provision of healthcare across the prison estate was assessed and commissioned.
1.5.2 HNAs are initiated and commissioned by NHS England regional teams; the reports are provided to the regional teams with findings and recommendations for healthcare provision. To bring a more standardised approach to the assessment process across the country, national guidance was produced in the form of the Health and Justice Health Needs Assessment Toolkit For Prescribed Places of Detention (referred to in this report as the Health and Justice Needs Assessment Toolkit) (Public Health England, 2014).
1.6 Equality Act 2010
1.6.1 The Equality Human Rights Commission (EHRC, 2018) described that it is the duty of a public service to anticipate reasonable adjustments for someone experiencing a physical or mental disability and ensure they are provided on an ongoing basis. This is so the person has equal access to services as someone without a disability and the same level of care.
1.6.2 The EHRC told HSSIB that an organisation must consider the equality impact of their policies to ensure they do not disadvantage people with a protected characteristic, which includes a mental disability. The EHRC (EHRC, 2024) have produced guidance to help organisations consider equality in policy making.
2. Analysis and findings
This section describes the investigation’s findings in relation to health needs assessments for prison populations and access for physically disabled people within prisons. These areas were identified during the evidence gathering phase for the three previous HSSIB reports within this series of work: emergency care response, continuity of care, and data sharing and IT.
This section includes experiences of disabled people in prison, specifically wheelchair users. The investigation observed some of the issues, and heard about them directly from people in prison and prison staff.
More information about the investigation’s evidence gathering and analysis can be found in the appendix.
2.1 Health needs assessments
2.1.1 NHS England regional teams initiate health needs assessments (HNAs) by contracting an external company to visit the relevant prison and carry out the assessment. To do this, the contracted company would commonly:
- observe the healthcare departments
- speak to people in prison
- assess the needs of people and patients in prison
- develop a draft report
- take feedback on the draft from the NHS England regional team
- produce a final written report.
Prison healthcare teams and companies undertaking the HNAs said this process took around 3 months to complete.
2.1.2 A template for HNAs was developed by Public Health England in 2014, when the assessments were introduced. Commissioners, providers and national organisations referred to this template as still commonly used as a basis for HNAs (Public Health England, 2014).
2.1.3 The national NHS England Health and Justice team had started reviewing HNAs in relation to their effectiveness for women’s prisons. The investigation was told that the current template, along with the “majority of policies and processes in prisons”, had been “designed around the male estate”, as men accounted for approximately 96% of all people detained in prisons in England.
2.1.4 A pilot version of a new HNA template for women’s prisons had been tested by some prisons and was being amended following feedback from the pilot sites. The investigation asked about future plans to review the template for the male estate, as the current version was more than 12 years old and had never been reviewed or amended. The team reviewing the HNA template for women’s prisons , led by the national NHS England Health and Justice team, said that there were “conversations required” about this next step, but they had considered it, even if plans were not yet in place to progress it.
Purpose of health needs assessments
2.1.5 Prison healthcare staff told the investigation that HNAs were used to assess the healthcare needs of the population of the prison and inform the commissioning of services offered by the healthcare provider.
2.1.6 The investigation reviewed the Health and Justice Health Needs Assessment Toolkit (Public Health England, 2014) and identified that HNAs are described as being relevant for a number of different stakeholders in the provision of healthcare. The organisations included local authorities, clinical commissioning groups (now ICBs) and those involved in offender management and support. The toolkit states that those carrying out HNAs should ‘consult interested stakeholders to make them aware of the work [HNA] and anticipate reception of the recommendations’. During conversations with NHS England regional teams, prison healthcare teams, and organisations that carry out HNAs, there was no mention of involving or consulting with these stakeholder groups as part of the HNA process.
2.1.7 While most of the healthcare providers and staff at national organisations referred to HNAs, some healthcare providers and commissioners referred to them as health and social care needs assessments (HSCNAs). The difference originated from the scope of the assessments, which also varied depending on the region. The investigation was told by healthcare providers and NHS England regional teams that some regions included assessment of social care needs as part of the process, while others only considered the health needs of the prison population. The NHS describes social care as ‘services to help you if you need practical support because of illness or disability’, which may include home adaptations, equipment to make life easier, personal alarms and monitoring systems and supported living services (NHS, 2024). HNAs are commissioned by NHS England regional teams and this was said to be the reason why some had decided not to include social care, which is outside of the remit of NHS England. All of the HNAs reviewed by the investigation included components of a social care needs assessment, although the depth of these assessments and subsequent recommendations were variable.
2.1.8 The investigation was also told by an organisation that conducts HNAs that it had seen examples where an NHS England regional team reviewed a draft HNA, which included social care needs, and asked the author to remove all the social care aspects because they were not the NHS regional team’s responsibility. There was no evidence to suggest that the information that was removed was fed back to the local authority to support their commissioning of social care for the prison.
2.1.9 The Health and Justice Health Needs Assessment Toolkit states that the ‘development and delivery’ of recommendations would be overseen by NHS England as the lead agency of an ‘HNA working group’. NHS England regional teams told the investigation that the incumbent “healthcare provider was responsible for the implementation of these” recommendations and that oversight of their implementation was variable. While the HNA would go to the prison partnership boards, there was no mention of an HNA working group and no collaborative working with other stakeholders, such as the local authority, on HNA recommendations.
2.1.10 The government’s 10 Year Plan for Health outlined the importance of local collaborative working to ensure health and social care delivery through ‘population health improvement plan[s]’, designed to ‘inform commissioning decisions’ within ICBs (UK Government, 2025). It is unclear if this will include how health and social care is delivered in prisons.
2.1.11 The investigation engaged with an NHS England regional team that had agreed with a local authority to co-commission the social care requirements for the prisons in its area. This had been achieved by using data available from the prison healthcare team to identify the social care needs and resource requirements within the prison. This then provided a cost comparison with what the local authority had commissioned. It was identified through this process that social care could be efficiently, and more cost effectively, delivered by the incumbent healthcare provider, which also gave some consistency in care provision for patients. The NHS England regional team told the investigation the arrangement had worked well and it was seeking to expand this arrangement to other local authorities in its region.
2.1.12 Aside from the above example, the investigation heard there was a separation between health and social care and a lack of clarity about the role of the HNA when planning services and identifying gaps. The lack of collaborative working between health and social care, and the impact this has on patients, has been identified in previous HSSIB reports (Health Services Safety Investigation Body, 2024; 2025a).
2.1.13 The separation of health and social care was found to cause frustration and uncertainty for people in prison. Healthcare staff described doing their best for patients, but largely social care was “out of their hands”.
Frequency of health needs assessments
2.1.14 The Health and Justice Needs Assessment Toolkit states:
‘A comprehensive HNA does not need to be undertaken every year. However, commissioners will need to assure themselves that their evidence-based priorities are up to date to inform the relevant local commissioning plans. If prisons are “re-rolled” [see 2.1.22], changing function and demographics this should prompt an updating of the HNA. To be transparent and enable wide participation, it is recommended that a full HNA should be completed at least once every 3 years with a refresh taking place within this time as relevant, e.g. when there is a change in population type. Thematic HNAs may also take place during this time depending on local need.’ (Public Health England, 2014)
2.1.15 Healthcare staff understood that HNAs could be triggered by specific events such as contract renewals, but should be carried out about every 3 years in any event. However, some healthcare providers were only able to provide the investigation with an HNA which was outside of this timeframe, or were unaware of when the last assessment had been carried out.
2.1.16 The investigation engaged with a company that had conducted many HNA assessments over a number of years. It described variation in the frequency of HNAs across the country depending on the NHS England regional teams. The company said that “best practice” was a full HNA being conducted every 3 years, with an annual update, usually conducted as a desktop review, to ensure that the assessment was still relevant and appropriate.
2.1.17 However, although some NHS England regional teams did request the 3-yearly assessments, annual reviews did not always take place. The company stated that this would depend on how “on the ball” the regional team was and whether the reviews formed part of an ongoing contract. The company was the first organisation to inform the investigation of annual reviews, even though it was one of the last organisations engaged with, demonstrating how rarely they were being conducted.
2.1.18 One healthcare provider told the investigation that some of the prisons it provided healthcare to had not had an HNA in more than 6 years. This created issues for the provider when assessing its service and trying to ensure that it was providing the care its patients required, as well as securing funding for continuation of that care.
2.1.19 The prisons visited by the investigation had differing experiences of HNAs and their frequency. For some, an HNA had been conducted during the same year, while others stated it had been a number of years since one had been completed. One prison commented that it had “sent in the forms” the previous year and 7 months later had not seen the final assessment. This did not necessarily mean that the HNA had not been completed, but that the healthcare department had not been provided with a copy of it. This could be explained by a comment made to the investigation by a company that carries out HNAs. It said that the completed documents were sent to the NHS England regional team, as the commissioner of the assessment, but the company was aware that they were not always sent on to the healthcare provider.
2.1.20 The investigation was told that even when HNAs were completed within the expected timeframes there were concerns about their efficacy. Many providers stated that HNAs were only a snapshot in time and were “only accurate on the day they were printed”. This was also identified in the Chief Medical Officers report, which stated, ‘[HNAs] are often outdated on publication. This results in inadequate understanding of the immediate and evolving health needs of the prison population...’ (HM Government, 2025)
2.1.21 For example, one prison healthcare provider said it had to rely on an HNA completed in 2021 to specify the commissioning requirements for a healthcare contract signed in 2023. The head of healthcare described the 2-year-old HNA as “not matching the needs” of the patient population by the time they took over the contract and the provision of care based on this information was therefore “difficult”. This was reflected by another provider which told the investigation that when taking over a service on change of contract that does not have a new HNA, the provider has to “take over and see what you’ve got”. The provider stated that “unless you are the incumbent provider you can’t assess the needs” before the commencement of the contract. They said that “[you are] finding your own way through the dark”.
2.1.22 A head of healthcare told the investigation that the population of their prison had changed dramatically in the last 12 months. The needs assessment did not reflect the current population and the provider had needed to submit multiple business cases to change the service it was providing. This situation was exacerbated if there were significant changes to the prison population, such as a change of category or being made specific to a particular cohort of prisoners, commonly termed a prison ‘re-role’.
2.1.23 Similarly, commissioners and healthcare providers told the investigation that reception prisons could not anticipate their healthcare requirements because of their rapidly changing populations. HNAs were described as less useful for these prisons, some of which had a change in population “every 28 days”. Some NHS England regional teams were using regularly reported local data to understand health needs (this is explored further in the section on other methods of assessing health needs, see 2.1.37).
2.1.24 The investigation was told that there was a need for a more reactive, flexible way to assess a prison’s healthcare requirements as its population changes. The investigation was also told of concerns about the costs of commissioning HNAs when they were considered by many to add little value. One commissioner told the investigation that each HNA cost approximately £10,000. Another said that “interchangeable populations and fast flow do not allow steady ground to spend £200K on HNAs”. Other methods of assessing health needs are explored further at 2.1.37 below.
Healthcare delivery
2.1.25 The investigation learned that when healthcare service delivery did not match the requirements set out in the healthcare provider contract, additional services or increased funding may be needed to deliver the required services.
2.1.26 The investigation was told that there were two main methods for amending the services provided to patients:
- submission of a business case to the NHS England regional team, detailing the service that needed amending, the reasons for the changes and the cost of the service change
- the healthcare provider adapting, changing the service and absorbing the cost of the change themselves if the change cannot be made within the current contract arrangement.
2.1.27 Business cases were described as being a “slow and laborious” process, and not reactive enough for services to change as quickly as the needs of patients in prisons. This meant that the services patients needed may not be in place, which may cause a delay in the delivery of their healthcare.
2.1.28 Information provided to the investigation showed that for the year 2024/25, amendments to healthcare contracts/services within the prison estate cost approximately £8m. These costs represented business case approvals and agreed payments to fund a prison re-role (see 2.1.22). What these costs do not show is how many business cases were submitted by healthcare providers and not agreed by commissioners, which may be the correct commissioning decision, and therefore not funded.
2.1.29 The experience of providers varied depending on the NHS England regional team that commissioned their services and the pressure the services were under. One provider told the investigation they were “unlikely to find a kind ear” when requesting more money for a service change, this was not an uncommon view across providers. In these cases the provider stated that, the service would either not be changed or the provider would absorb the costs of the change. If it was unable to do so, patients would not receive the care they needed.
2.1.30 The investigation was told there was a reliance on healthcare providers to adapt and absorb the costs of services. An NHS England regional team said that if a healthcare provider could react to a changing healthcare need and there was no cost involved then it would expect that to happen.
2.1.31 The investigation was given examples where the role of the prison had been changed, which impacted on the healthcare services required by that prison population. In one case, a prison that formerly housed prisoners of mixed age had been changed to housing mostly vulnerable prisoners (people convicted of sexual offences). These prisoners were described, by national organisations, healthcare providers and prison staff, as typically older people, many with greater social care and age-related health needs. They also had less need for other services which had been previously required, such as substance misuse services. The prison involved said no HNA had been carried out in response to this significant change and the healthcare provider was given “very little warning”. This was not an isolated incident and other providers, along with regional commissioners, in similar situations said they were also given “little, to no warning” of a prison re-role. The healthcare providers stated that there was an expectation they would adapt to the needs of patient cohorts as they changed, but that this could take time and there may be a delay in offering the required services. This could result in the potential for patient harm.
2.1.32 HM Prison and Probation Service (HMPPS) told the investigation that any considerations around “introducing a new population” to a prison were discussed at the national Custodial Capacity Board. These meeting were attended by representatives from the NHS England Health and Justice national team. However, HMPPS said in its experience the implications of discussions at the Custodial Capacity Board did not always reach the NHS England regional teams or the local healthcare providers that would be affected.
2.1.33 HMPPS explained that in recognition of gaps in communication it had attempted to engage with local healthcare providers and NHS England regional teams in discussions about population changes. This was to ensure that providers and commissioners were aware of the potential for changes in service requirements. Following these engagements, HMPPS stated that it had received feedback that these discussions needed to involve the NHS England Health and Justice national team.
2.1.34 The NHS England Health and Justice national team told the investigation that it was aware that often regional teams and healthcare providers were not informed in sufficient time to change their services to the needs of a new cohort of patients. Changes providers might need to make included;
- training staff in new aspects of healthcare
- employing staff into different roles and possibly reducing/increasing certain roles (for example, substance misuse nurses, mental health nurses, healthcare assistants)
- recruiting staff.
These changes required time, planning and sometimes additional funds.
2.1.35 The NHS England Health and Justice national team stated that attendance at the Custodial Capacity Board was a reasonably new development. An issue arising from the meeting was that insufficient detail was provided for healthcare planning and costing was not possible at this point. Once changes to the patient cohort had been confirmed and permission was granted to pass the details to the regional teams, there was often not much time left until the changes happened. The healthcare department had regularly been advised of the change by the prison governor by this time.
2.1.36 The investigation identified a gap in communication between prison healthcare teams, HMPPS and NHS England national and regional teams. With the potential for NHS England national and regional teams to be separated, with the national team moving into the Department of Health and Social Care and the regional teams becoming part of integrated care systems, there is a need to create robust communication routes between the national Custodial Capacity Board and prison healthcare providers via the regional teams.
HSSIB makes the following safety recommendation
Safety recommendation R/2026/079:
HSSIB recommends that HM Prison and Probation Service, in collaboration with the Department of Health and Social Care, formalises arrangements for alerting healthcare commissioners and providers to changes in prison populations likely to impact on healthcare provision requirements. This is to ensure that healthcare commissioners and providers can plan for changes to healthcare services that are necessary to meet the changing needs of the prison population.
Other methods of assessing health needs
2.1.37 Prison healthcare staff had differing opinions about the usefulness of HNAs and the value they added. Healthcare providers (that served several prisons), regional teams and national stakeholders felt that HNAs added little value because they became out of date as soon as they were finalised.
2.1.38 NHS England regional teams and prison healthcare providers told the investigation they wanted a more reactive and flexible way of providing the right care provision to patients, which the constraints of the current system did not allow. While some regional teams were continuing with the standard process, as outlined at 2.1.1, others had developed different approaches in response to the recognised need for a more current picture of the health needs of patients in prison. The investigation spoke to two regions that were using different methods to assess the needs of their prison populations.
2.1.39 One NHS England regional team had stopped using HNAs completely and was using data gathered through other means to review healthcare requirements. It gathered the data through multiple existing sources which included:
- monthly provider returns
- monthly performance reviews
- quality assurance visits
- clinical quality review meetings
- regular prison expansion meetings
- local authority social care meetings.
This data was then pulled into a dashboard to enable a monthly view of the prison population and its needs. The regional team acknowledged that this system did not always capture data of the required specificity. It indicated there was more work to be done, but that this system provided a much more current view of the prison’s healthcare needs, and was available a few days after the data was submitted. It was working with another NHS England regional team to enable a comparison across prisons with similar patient cohorts to assess service requirements, to ensure efficiency and effectiveness. It indicated that in future this could be used to support changes in service provision requirements when a prison was re-roled.
2.1.40 Another NHS England region was trialling an approach which stemmed from a data quality and improvement programme for performance data. This project had enabled the regional team’s IT provider to be granted access to the healthcare IT systems. It was identified that relevant data could be pulled from these systems to understand the healthcare needs of the prison population, rather than commissioning an HNA. This live access to the data enabled a real-time view of health needs, as well as the development of live dashboards and the ability to look at historical data and trends. The regional team also told the investigation that in the event of a planned re-role of one of its prisons, for example from a male prison to a female prison, it could use live data gathered from other similar prisons to assist with designing the healthcare provision.
2.1.41 The regional team had developed an artificial intelligence (AI) HNA assessment tool which pulled data to enable a full report to be prepared, and triggered events including patient engagement, which it then incorporated into the needs assessment. The regional team described this system as a “game changer to monitor current health needs” and there were plans to incorporate social care needs into the system in the future. The team said that moving to this system had halved the costs of creating an HNA.
2.1.42 The NHSE regional teams felt the need to deviate from the current HNA process because in their view it did not enable timely assessment of the healthcare needs of prison populations, and therefore did not enable regional teams and healthcare providers to respond to changes. The investigation learned that the innovations described above had been developed in isolation of each other and several NHS England regional teams stated they were “not great at inter region working”, which “only really happens when there is a problem”. There was recognition that some of the innovations could be rolled out nationally, but because NHS England regional teams were responsible for commissioning services for the prisons in their area, there appeared to be little oversight or requirement for a uniform approach across regions. Prison healthcare providers that covered multiple regions and therefore worked with different NHS England regional teams told the investigation there was no consistency of approach across regions. This led to variability in how healthcare was delivered to patients across regions, and the timeliness of contract changes to reflect changes in the needs of patient populations.
2.1.43 The investigation notes that there is a national approach to the development of HNAs, initially for women’s prisons, but this has been superseded in some areas by regional projects in response to recognised challenges with the HNA process. While most national, regional and local stakeholders considered the HNA process as it stands to be inefficient and to have the potential to impact on care delivery, variability across regions also caused challenges. There is a clear need for change in the methods of assessing the healthcare needs for people in prison, a process which should involve; people in prison, prison healthcare providers and staff, as well as the commissioning teams and local authorities.
2.1.44 Given the rapidly changing landscape in healthcare and the changes to NHS England, the following safety recommendation has been developed and must be considered once governance arrangements have been finalised.
HSSIB makes the following safety recommendation
Safety recommendation R/2026/080:
HSSIB recommends that the Department of Health and Social Care works with local authorities to redesign how the health and social care needs of prisons’ populations are assessed. This is to ensure that appropriate services are commissioned to meet the needs of people in prison and prevent possible delays in care.
2.2 Physical disability access
Number of wheelchair users
2.2.1 In the general population of England, adult wheelchair users make up approximately 1% of the population (585,732). This information is taken from the National Wheelchair Data Collection dataset (NHS England, 2025) and the Office for National Statistics population data for mid-2024 (Office for National Statistics, 2025).
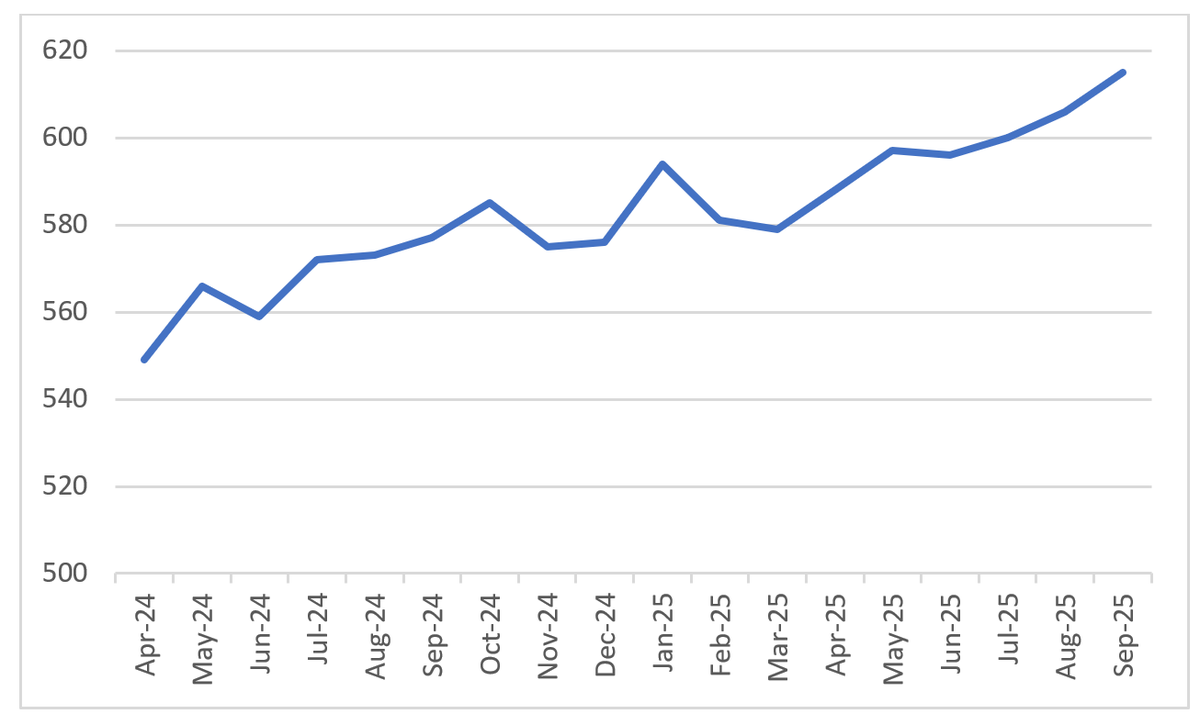
2.2.2 In men’s prisons approximately 0.8% of the population are wheelchair users (615); however, this figure is increasing and appears to mirror the increasing age of the prison population. Figure 1 shows the increase in wheelchair users over time.
Figure 1 Number of wheelchair users in prison in England
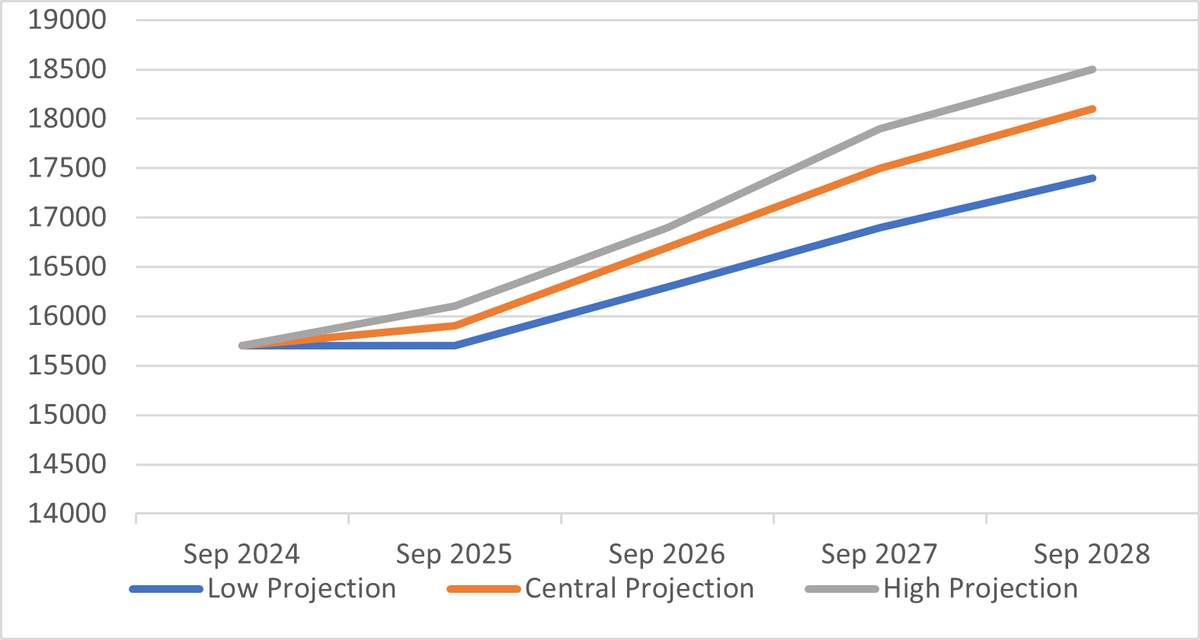
2.2.3 The prison population is increasing, as is the average age of people in prison. Figure 2 shows government projections for the number of people in prison who are over the age of 50 up to September 2028, including low, central and high projections.
Figure 2 Government projected numbers of people aged over 50 in the detained estate
2.2.4 The investigation was told that much of the prison estate was old and not built to accommodate the needs of older people or wheelchair users. In addition, the increasing social care needs of an ageing prison population had posed challenges for prisons in providing adequate accommodation and appropriate care for older people and wheelchair users.
Accessible cells
2.2.5 Prison healthcare staff described cells as ‘wheelchair accessible’, ‘accessible or adapted’, and ‘standard’. Accessible cells may have wider doors, handrails and alarm cords to assist people as needed. During the investigation’s site visits, concern was raised by people in prison and healthcare staff about the number of wheelchair accessible cells. None of the prisons visited said that they had enough cells to accommodate every wheelchair user in a wheelchair accessible cell. HMPPS responded to the investigation stating that there were several categories of cells which included:
- accessible
- low mobility
- end of life care
- health or medical cells
- cells with adaptations.
2.2.6 One NHS England regional team told the investigation it had 6,000 cells across its region, not one of which was a wheelchair accessible cell. The investigation was told several times that some wheelchair users were accommodated in cells that were accessible, but were not classed as wheelchair accessible.
2.2.7 At the prisons visited, the proportion of wheelchair accessible cells ranged from 0.1% to 0.75%. The older prisons had fewer wheelchair accessible cells – between 0.1% and 0.2% – while the newer prisons had between 0.6% and 0.75%. These figures are all below both the national average of wheelchair users and the average for the prison population. One prison told the investigation that it had six wheelchair accessible cells and two adapted cells that were suitable for people with mobility issues (who had difficulty walking but could walk) but, according to data supplied by NHS England, it had 20 wheelchair users.
2.2.8 HMPPS told the investigation that prisons communicated with each other through their Offender Management Units to agree transfers of wheelchair users. They stated that prisons would only accept wheelchair users if there was suitable accommodation for them at that prison. However, multiple healthcare teams stated that, if patients who had been transferred to hospital needed a change in accommodation, due to illness or disability, it was often left to the healthcare department to try and find them suitable accommodation. The investigation heard this was not the experience of every prison, with some prison healthcare teams describing cases where they highlighted they did not have the accommodation for a certain individual’s needs, but the person was still transferred to them.
Impact on disabled people and those with limited mobility
2.2.9 During site visits the investigation observed several people moving around prisons in their wheelchairs, with one person demonstrating how they accessed their cell. The cell door was not wide enough for their wheelchair to pass through, so a second wheelchair had been dismantled and rebuilt inside the cell. The person reported often having to self‑transfer between the external and internal wheelchair, with a gap of approximately 2 to 3 feet between chairs. They would “regularly fall between the chairs”, sustaining minor injuries (cuts and bruises). Assistance from staff or other prisoners to move from chair to chair was inconsistent and the person often did so independently.
2.2.10 A member of staff from a healthcare department told the investigation about a patient who was predominantly bed bound, but could be moved around the prison in a wheelchair. The prison did not have any wheelchair accessible cells or cells that were either accessible or adapted to suit his needs. Because of this he had been accommodated in the healthcare department, but the only space available was in the palliative care ward. He had been living there for several months. The staff member told the investigation that the patient’s mental health had deteriorated, because he was on a ward with patients who were dying and had no meaningful activities or interactions each day, and that he had started to self-harm.
2.2.11 There were many examples of prisons that had wheelchair accessible cells; however, these cells were not always appropriately located. One prison told the investigation that they had six wheelchair accessible cells, but they were all on the vulnerable prisoner (people convicted of sexual offences) wing. This had caused issues for people in wheelchairs who were not vulnerable prisoners as they had then been wrongly associated as such by the rest of the prison population.
2.2.12 The investigation heard that there were also issues with the availability of accessible and adapted cells in prisons. One example was where accessible cells, used for people who were less mobile, were located on an upper level of the wing. The cells’ occupants had to climb stairs to access the upper floors and found this difficult, often needing assistance.
2.2.13 Evidence gathered from the prisons the investigation visited suggested that the shortage of suitable cells for wheelchair users across the detained estate was causing patient harm.
Prison expansion plans
2.2.14 In December 2024 the government published its 10-year prison expansion strategy, which sought to address capacity issues by expanding prisons and building new estates. The strategy does not openly mention disability or accessibility as part of the planned developments. However, HMPPS told the investigation that all new cells built as part of the expansion plan would be “accessible by design”. NHS England regional teams also told the investigation there was “lots being done as part of the expansion programme” in relation to disability access.
2.2.15 HMPPS described new wings being developed which included low mobility cells and others which included the use of “modular accommodation”, which was wheelchair accessible. NHS England regional teams told the investigation that such improvements would benefit older, frailer people in prison. However, it was acknowledged that some improvements may be set aside for people convicted of sexual offences as the cohort most commonly requiring such adaptations.
2.2.16 Some national stakeholders suggested there may need to be some “cohorting” of wheelchair users into prisons designed, or adapted, for their needs. HMPPS stated that, with the extent of the expansion plans and the accessible by design concept, this was not likely to be required. However, while the expansion plan is being implemented there will still be a shortage of cells across the prison estate, with some areas more affected than others. Some stakeholders expressed concern that placing people in suitable accommodation far from their intended resettlement area could negatively affect their rehabilitation.
2.2.17 In 2024 HMPPS produced a guide to support the allocation of adapted cells. This mapped the types of accessible cell available across the prison estate, their locations and the healthcare provision within those prisons. HMPPS also established a working group to improve access to adapted cells within the private prison estate, where the highest concentration of such cells were located.
2.2.18 Although this work improved understanding of adapted cell availability, HMPPS said incomplete data on the needs of people in prison continued to make it difficult to place wheelchair users and others with limited mobility. It also stated that issues arose due to healthcare staff not wanting to share information for fear of breaking medical confidentiality. This included information which would assist in identifying suitable accommodation for individuals. The knock-on effect of this was that it blocked the flow of people with specific accommodation needs from reception prisons to the training and resettlement prisons. This was because reception prisons had no choice but to accept wheelchair users arriving on remand or from court. However, training and resettlement prisons could refuse to accept the transfer of people with specific accommodation requirements if they could not meet these requirements.
2.2.19 While the expansion of prison accommodation is forecast to meet the needs of the rising number of wheelchair users in prison, this increased capacity is not an immediate or short-term solution for those currently in prison. During the time the expansion strategy is being implemented, the accommodation that is available must be used efficiently to reduce the number of wheelchair users in unsuitable cells. In order to manage this, the system of accommodation allocation needs more reliable data on the needs of disabled people in relation to accommodation requirements.
2.2.20 HMPPS told the investigation that the data it was given by healthcare departments on whether an individual had a physical disability was not “consistent or validated”. It stated that substantiated data would assist with understanding where someone could or could not be housed. Although this suggests that the provision of this data was only possible via healthcare departments, the Ministry of Justice ‘Advancing equality for offenders and children in custody policy framework’ states:
‘Details pertaining to protected characteristics [including physical disability] must be collected and recorded at the earliest opportunity and for every new event. At Court; first Probation appointment or induction into custody via the Diversity & Inclusion Form (DIF14). This information is self-disclosed and as new protected characteristic information is given, the appropriate data collection management information system must be updated.’ (Ministry of Justice, 2024b)
2.2.21 HMPPS also described a workaround it was currently using to try and identify individuals’ accommodation needs using personal evacuation plans (plans for people who need assistance during an emergency).
2.2.22 While the evidence shows that frameworks have been written to support the collection of data including physical disabilities, the data collection systems are not functioning efficiently or effectively. This demonstrates a disconnect between expectations regarding whose role it is to gather and record this information.
2.2.23 In a previous HSSIB, report, ‘Healthcare provision in prisons: data sharing and IT’ (Health Services Safety Investigations Body, 2025b), safety recommendations were made to both HMPPS and NHS England to ensure that any new IT system should support interoperability between the prison management system and the healthcare system. These safety recommendations were specifically aimed at sharing data that did not breach the confidentiality and security requirements of each organisation.
2.2.24 If data about accommodation requirements was shareable, HMPPS would be able to identify more easily the accommodation requirements for wheelchair users and people with limited mobility. This would then allow it to improve the flow and management of limited resources to support wheelchair users or people with accessibility needs.
2.2.25 In the long term, HSSIB’s safety recommendation made would assist with the identified information disconnect. However, until the safety recommendation is fully implemented there remains a misalignment between ‘work as prescribed’ and ‘work as done’.
2.2.26 Due to its previous safety recommendation, HSSIB does not intend to make a further safety recommendation in this area. However, HSSIB highlights the importance of this safety recommendation to the welfare of people in prison and the ability of HMPPS to comply with its ‘Advancing equality for offenders and children in custody policy framework’. This would likely reduce the risk of harm and improve the efficiency with which HMPPS can place people in suitable accommodation.
HSSIB makes the following safety recommendation
Safety recommendation R/2026/081:
HSSIB recommends that HM Prison and Probation Service reviews and amends its information gathering processes for accommodation requirements for wheelchair users and people with mobility issues, to identify and mitigate risks for people whose accommodation does not meet their needs. This is to enable and support the effective identification of appropriate prison accommodation for these groups.
3. References
Equality and Human Rights Commission (2018) Terms used in the Equality Act 2010. Available at https://www.equalityhumanrights.com/equality/equality-act-2010/your-rights-under-equality-act-2010/terms-used-equality-act (Accessed 17 March 2025).
Equality and Human Rights Commission (2024) How to consider equality in policy making: A 10-step guide for public bodies in England. Available at https://www.equalityhumanrights.com/guidance/how-consider-equality-policy-making-10-step-guide-public-bodies-england (Accessed 17 March 2026).
Health Services Safety Investigations Body (2024) Mental health inpatient settings: supporting safe care during transition from inpatient children and young people’s mental health services to adult mental health services. Available at https://www.hssib.org.uk/patient-safety-investigations/mental-health-inpatient-settings/third-investigation-report/ (Accessed 5 January 2026).
Health Services Safety Investigation Body (2025a) Workforce and patient safety: primary and community care co-ordination for people with long-term conditions. Available at https://www.hssib.org.uk/patient-safety-investigations/workforce-and-patient-safety/fourth-investigation-report/ (Accessed 5 November 2025).
Health Services Safety Investigation Body (2025b) Healthcare provision in prisons: data sharing and IT. Available at https://www.hssib.org.uk/patient-safety-investigations/healthcare-provision-in-prisons/third-investigation-report/ (Accessed 6 Jan 2026).
Healthcare Safety Investigation Branch (2019) Management of chronic health conditions in prisons. Available at https://www.hssib.org.uk/patient-safety-investigations/management-of-chronic-health-conditions-in-prisons/ (Accessed 28 May 2025).
HM Government (2025) The health of people in prison, on probation and in the secure NHS estate in England. Available at https://assets.publishing.service.gov.uk/media/690b6f65c22e4ed8b0518515/full-report-chief-medical-officer-health-of-prisoners-accessible.pdf (accessed 9 March 2026).
House of Commons Health and Social Care Committee (2018) Prison health. Available at https://publications.parliament.uk/pa/cm201719/cmselect/cmhealth/963/963.pdf (Accessed 17 June 2024).
Ministry of Justice (n.d.a) About us. Available at https://www.gov.uk/government/organisations/ministry-of-justice/about (Accessed 7 May 2024).
Ministry of Justice (n.d.b) Working in the prison and probation service. Your A-D guide on prison categories. Available at https://prisonjobs.blog.gov.uk/your-a-d-guide-on-prison-categories/ (Accessed 10 April 2024).
Ministry of Justice (2024a) 10-year prison capacity strategy. Available at https://assets.publishing.service.gov.uk/media/67586f828a1ef8f66413b9c2/24.231_MOJ_10-Year_Capacity_Strat_Pub_v10.1_WEB.pdf (Accessed 5 November 2025).
Ministry of Justice (2024b) Advancing equality for offenders and children in custody policy framework. Available at https://assets.publishing.service.gov.uk/media/670fc363366f494ab2e7b9db/advancing-equality-offenders-children-policy-framework.pdf (Accessed 12 January 2026).
NHS (2024) Introduction to care and support. Available at https://www.nhs.uk/social-care-and-support/introduction-to-care-and-support/ (Accessed 19 January 2026).
NHS England (2025) Wheelchair data collection. Available at https://www.england.nhs.uk/statistics/statistical-work-areas/national-wheelchair/ (Accessed 26 November 2025).
Office for National Statistics (2025) Estimates of the population for the UK, England, Wales, Scotland, and Northern Ireland. Available at https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/datasets/populationestimatesforukenglandandwalesscotlandandnorthernireland (Accessed 26 November 2025).
Public Health England (2014) Health and Justice Health Needs Assessment Toolkit for Prescribed Places of Detention. Available at https://assets.publishing.service.gov.uk/media/5c51711740f0b625504f4591/Health_Needs_Assessment_Toolkit_for_Prescribed_Places_of_Detention_Part_1.pdf (Accessed 20 November 2025).
Royal College of General Practitioners (2018) Equivalence of care in secure environments. Available at https://www.rcgp.org.uk/representing-you/policy-areas/care-in-secure-environments (Accessed 30 June 2025).
The King’s Fund (2025) NHS regions – what do they do and how are they changing? Available at https://www.kingsfund.org.uk/insight-and-analysis/blogs/nhs-regions?utm_term=thekingsfund&utm_source=linkedin&utm_medium=social (Accessed 19 January 2026).
UK Government (2025) Fit for the future. 10 Year Health Plan for England. Available at https://assets.publishing.service.gov.uk/media/6888a0b1a11f85999 4409147/fit-for-the-future-10-year-health-plan-for-england.pdf (Accessed 5 January 2026).
4. Appendix
Investigation approach
The investigation report ‘Management of chronic conditions in prisons’ (Healthcare Safety Investigation Branch, 2019) identified areas of healthcare which were out of scope for that investigation that would likely warrant an investigation. To identify topics for investigation within the healthcare provision in prisons theme, the investigation reviewed intelligence from service and professional regulators, national reports, academia and research. Discussions also took place with a large number of national stakeholders to understand their concerns in this area.
Evidence was collated and analysed to identify common areas across the stakeholders which were directly related to patient safety concerns. Each area was then placed into a hierarchy based on the number of stakeholders raising it, the breadth of the concern across the prison estate, whether it affected male and female prisons and the estimated seriousness of the concern. As a result of this work the investigation was formally launched in February 2024 looking at three main topics:
- emergency care response
- continuity of care
- data sharing and IT.
During the evidence gathering for these investigations, issues were identified which did not fall within their terms of reference. Due to the prevalence of these issues and following discussions during HSSIB governance meetings it was agreed to produce a fourth report relating to physical healthcare in prisons to explore the topics of needs assessments and physical disability access.
Evidence gathering
The investigation carried out a programme of visits that was designed to be as efficient as possible and to account for all aspects of the prison estate, covering all three topics listed above. All the evidence was grouped into the different topic areas for analysis.
The investigation’s site visits covered:
- category A to D prisons (male) and closed prisons (female)
- prison buildings of a range of ages (1800s to 2020s)
- four geographical areas across England (south-east, midlands, north-west, north-east)
- three prison operators
- four prison healthcare providers.
The investigation engaged with:
- prison officers and security staff
- prison management
- national and local commissioners
- healthcare staff and healthcare provider management.
All evidence collection was carried out using standardised question sets for each visit and interview, enabling a like-for-like analysis of healthcare provision across prisons in England. Evidence was coded into key lines of inquiry and subject areas. Once coded, the evidence was thematically analysed by the investigation team, ensuring strength and breadth of evidence was assured. The analysis was independently reviewed to ensure the evidence directly led to the findings and safety recommendations reflected in the report.
Stakeholder engagement and consultation
The investigation engaged with the following stakeholders to gather evidence and check for factual accuracy, and for overall sense-checking. The stakeholders contributed to the development of the safety recommendations based on the evidence gathered.
| National organisations | Other organisations |
|---|---|
| HM Prison and Probation Service | Observations at 13 prisons and engagement with an additional 3 |
| NHS England | Prison healthcare providers |
| Ministry of Justice | ABL Health |
| Health needs assessment provider |